



Abstract
This article describes the case of a deaf native signer of American Sign Language (ASL) with a specific language impairment (SLI). School records documented normal cognitive development but atypical language development. Data include school records; interviews with the child, his mother, and school professionals; ASL and English evaluations; and a comprehensive neuropsychological and psychoeducational evaluation, and they span an approximate period of 7.5 years (11;10–19;6) including scores from school records (11;10–16;5) and a 3.5-year period (15;10–19;6) during which we collected linguistic and neuropsychological data. Results revealed that this student has average intelligence, intact visual perceptual skills, visuospatial skills, and motor skills but demonstrates challenges with some memory and sequential processing tasks. Scores from ASL testing signaled language impairment and marked difficulty with fingerspelling. The student also had significant deficits in English vocabulary, spelling, reading comprehension, reading fluency, and writing. Accepted SLI diagnostic criteria exclude deaf individuals from an SLI diagnosis, but the authors propose modified criteria in this work. The results of this study have practical implications for professionals including school psychologists, speech language pathologists, and ASL specialists. The results also support the theoretical argument that SLI can be evident regardless of the modality in which it is communicated.
In recent years, descriptions of deaf children who exhibit developmental language disorder within the visual–gestural modality have begun to appear (Marshall, Denmark, & Morgan, 2006; Marshall, Rowley, Mason, Herman, & Morgan, 2013; Marshall et al., 2015; Marshall & Morgan, 2016; Mason et al., 2010; Morgan, Herman, & Woll 2007; Quinto-Pozos, Forber-Pratt, & Singleton, 2011; Quinto-Pozos et al., 2013). Unfortunately, signed language disorders have traditionally not been considered within various theoretical approaches to developmental communication disorders (see Quinto-Pozos, 2014 for a discussion). One challenge for educators, clinicians, and researchers who consider language development in signing deaf children is that assessment tools and diagnostic criteria have traditionally focused on spoken language development. Yet, investigations of atypical acquisition of a signed (i.e., visual–gestural) language permit researchers to consider whether some types of communication disorders can appear across linguistic modalities (i.e., both auditory–oral and visual–gestural) and whether some disorders might be unique to the channels in which they are communicated. The study of signed language impairments is an important prerequisite for the assessment, diagnosis, and treatment of developmental language disorders among deaf children.
As a starting point for understanding the characteristics of deaf children with language impairment, Quinto-Pozos et al. (2011) interviewed school professionals at ASL–English bilingual schools. They focused on the language development of deaf native signers who were born to and raised by deaf signing parents. This is important because previous research has found that deaf native signers achieve language developmental milestones at the same rate as hearing speakers do in spoken languages (Newport & Meier, 1985; Petitto et al., 2001). Quinto-Pozos and colleagues asked teachers, speech language pathologists, and school psychologists if they had observed deaf native signers in their school exhibiting atypical patterns of ASL production or comprehension compared to other native signers of the same age. All interviews were conducted in ASL (whether the interviewees were deaf or hearing), and all interviewees could communicate fluently.
School professionals did not hesitate to describe cases of atypicality that they had observed over the years. They gave reports of signed stuttering, production errors involving facial cues, comprehension difficulties, errors in use of space, difficulties with sign phonology, failures in establishing reference information (e.g., time, place, and referents), and atypical switching of hand dominance. Regarding the prevalence of sign-based atypicality among the signers they had interacted with, one interviewee said that she has only seen about five native signers appearing to exhibit atypicality with aspects of their ASL (production and/or comprehension) in 18 years of working with children who are deaf or hard of hearing (D/HH). Another professional estimated that he normally sees one new child per academic year, but he also felt that it used to be fewer—about one every 3 years. One professional felt that such sign-based deficits were evident in only 1 out of the 12 children at that school who were native signers. In total, focus groups that consisted of mostly speech and language pathologists suggested that the incidence of such deficits in native signing children is approximately 3–5% (Quinto-Pozos et al., 2011).1
Studies of British Sign Language (BSL) have proposed that some signing deaf children in the UK exhibit symptoms of a sign-based SLI (Marshall et al., 2006, 2013, 2015; Mason et al., 2010; Morgan et al., 2007). In the first report of its kind, Morgan & colleagues (2007) described various characteristics of “Paul,” a native signing deaf child (age 5.2 years), with typical cognitive development and no visual or motor difficulties, who struggled with multiple BSL linguistic constructions including negation, noun–verb sign pairs (i.e., derivational morphology), and spatially modified verbs (i.e., inflectional morphology). Paul provided evidence that a native signer of a signed language can exhibit language impairment in the visual–manual modality, and complex morphological constructions could be susceptible to such a linguistic deficit. Later studies from the U.K. team of researchers involved groups of atypically developing children compared with typically developing (TD) peers. One of the first group studies of its kind was published in 2010 (Mason et al., 2010), which focused on a small group of deaf children with suspected sign-based SLIs using normed tests of BSL that included sentence comprehension, repetition of nonsense signs, expressive grammar, and narrative skills. The authors combined those assessments with tests of nonverbal intelligence and fine motor control. Their results confirmed that complex morphology may be among the most fragile aspects of signed language acquisition. Each child scored at least 1.3 SD below the mean on at least one BSL test, yet all met the criteria of being within the average range on tests of nonverbal cognitive ability. A 2013 study of semantic fluency (Marshall et al., 2013) revealed that SLI-diagnosed children performed similarly to their TD peers in multiple ways (which argues for a similar semantic organization of the signed lexicon across groups), but the SLI children were slower in providing responses, suggesting that their process of lexical access is less efficient than that of the TD children. Of particular interest to the present manuscript is the report of an SLI-diagnosed child who showed signs of fingerspelling challenges (e.g., by fingerspelling G-G-E-E instead of E-G-G when referring to an egg). The authors suggest that the error “…could reflect uncertainty with the phonology of the fingerspelt form and/or the orthography of the English word.” (213) Finally, two additional studies from the UK (Herman, Rowley, Mason & Morgan 2014; Marshall et al., 2015) highlight additional differences between SLI-diagnosed children and their TD peers. Herman and colleagues looked at narratives in BSL and showed that like the 2010 study, the SLI children performed poorly on verb morphology, and their narratives exhibited less structure and were shorter than those of the TD children. The other study (Marshall et al., 2015) focused on sentence repetition, which is also pertinent to this study. Their findings indicate that the SLI children were less able to accurately repeat all elements of BSL sentences, including individual signs, correct word order and grammatical constructions, and facial expressions. Taken together, the body of work that has emerged from the UK on BSL-signing children diagnosed with SLI indicates that atypicality in the sign modality shows many of the same characteristics as linguistic deficits in hearing children. Deaf children with SLI often struggle with complex morphology, their lexical processing is less efficient than their TD peers’ processing, their narratives are shorter and exhibit less structure than those from TD peers, and they are less able to accurately repeat all parts of a sentence repetition task.
The study, diagnosis, and treatment of sign-based language impairment is challenging partially due to the lack of a set of diagnostic criteria that is appropriate for use with signed language users. The diagnostic criteria for specific language impairment (SLI) that is widely used can be found in Leonard (1998, Table 1). Leonard notes that the diagnosis is primarily one of exclusion: a determination has to be made that other conditions do not generally co-occur with language deficit(s). This is a problem because deaf children are automatically excluded from a possible diagnosis because of their hearing status; all atypical language development by D/HH children would be secondary to their hearing status.
Criteria for Specific Language Impairment Diagnosis
| Factor | Criterion |
|---|---|
| Language ability | Language test scores of −1.25 SD or lower; at risk for social devalue |
| Nonverbal IQ | Performance IQ of 85 or higher |
| Hearing | Pass screening at conventional levels |
| Otitis media with effusion | No recent episodes |
| Neurological dysfunction | No evidence of seizure disorders, cerebral palsy, brain lesions; not under medication for control of seizures |
| Oral structure | No structural anomalies |
| Oral motor function | Pass screening using developmentally appropriate items |
| Physical and social interactions | No symptoms of impaired reciprocal social interaction or restriction of activities |
| Factor | Criterion |
|---|---|
| Language ability | Language test scores of −1.25 SD or lower; at risk for social devalue |
| Nonverbal IQ | Performance IQ of 85 or higher |
| Hearing | Pass screening at conventional levels |
| Otitis media with effusion | No recent episodes |
| Neurological dysfunction | No evidence of seizure disorders, cerebral palsy, brain lesions; not under medication for control of seizures |
| Oral structure | No structural anomalies |
| Oral motor function | Pass screening using developmentally appropriate items |
| Physical and social interactions | No symptoms of impaired reciprocal social interaction or restriction of activities |
Criteria for Specific Language Impairment Diagnosis
| Factor | Criterion |
|---|---|
| Language ability | Language test scores of −1.25 SD or lower; at risk for social devalue |
| Nonverbal IQ | Performance IQ of 85 or higher |
| Hearing | Pass screening at conventional levels |
| Otitis media with effusion | No recent episodes |
| Neurological dysfunction | No evidence of seizure disorders, cerebral palsy, brain lesions; not under medication for control of seizures |
| Oral structure | No structural anomalies |
| Oral motor function | Pass screening using developmentally appropriate items |
| Physical and social interactions | No symptoms of impaired reciprocal social interaction or restriction of activities |
| Factor | Criterion |
|---|---|
| Language ability | Language test scores of −1.25 SD or lower; at risk for social devalue |
| Nonverbal IQ | Performance IQ of 85 or higher |
| Hearing | Pass screening at conventional levels |
| Otitis media with effusion | No recent episodes |
| Neurological dysfunction | No evidence of seizure disorders, cerebral palsy, brain lesions; not under medication for control of seizures |
| Oral structure | No structural anomalies |
| Oral motor function | Pass screening using developmentally appropriate items |
| Physical and social interactions | No symptoms of impaired reciprocal social interaction or restriction of activities |
The authors adapted SLI diagnostic criteria of Leonard (1998) to address the case of deaf signing children. Specifically, two of the criteria concern hearing ability (“Hearing” and “Otitis media with effusion”) and two focus on speaking (“Oral structure” and “Oral motor function”) were replaced with visual abilities (for language reception and comprehension) and motor abilities that involve the articulators for signed language—such as the fingers, hands, arms, head, and torso (for language production). The proposed diagnostic criteria are described in Table 2; these were applied to the case of a deaf child in this study.
Proposed criteria for a signed language SLI diagnosis
| Factor | Criteria |
|---|---|
| Language ability | Exposure to fluent signers at home and school beginning early in life. Sign language test scores of −1.25 SD or lower; at risk for social devalue |
| Nonverbal IQ | Performance IQ of 85 or higher |
| Vision | No impairment beyond corrected with glasses or contacts |
| Neurological dysfunction | No evidence of seizure disorders, cerebral palsy, brain lesions; not under medication for control of seizures |
| Face, arm, hand, and finger structure | No structural anomalies that impede language production |
| Gross and fine motor function | No impairments that impede language production |
| Physical and social interactions | No symptoms of impaired reciprocal social interaction or restriction of activities |
| Factor | Criteria |
|---|---|
| Language ability | Exposure to fluent signers at home and school beginning early in life. Sign language test scores of −1.25 SD or lower; at risk for social devalue |
| Nonverbal IQ | Performance IQ of 85 or higher |
| Vision | No impairment beyond corrected with glasses or contacts |
| Neurological dysfunction | No evidence of seizure disorders, cerebral palsy, brain lesions; not under medication for control of seizures |
| Face, arm, hand, and finger structure | No structural anomalies that impede language production |
| Gross and fine motor function | No impairments that impede language production |
| Physical and social interactions | No symptoms of impaired reciprocal social interaction or restriction of activities |
Proposed criteria for a signed language SLI diagnosis
| Factor | Criteria |
|---|---|
| Language ability | Exposure to fluent signers at home and school beginning early in life. Sign language test scores of −1.25 SD or lower; at risk for social devalue |
| Nonverbal IQ | Performance IQ of 85 or higher |
| Vision | No impairment beyond corrected with glasses or contacts |
| Neurological dysfunction | No evidence of seizure disorders, cerebral palsy, brain lesions; not under medication for control of seizures |
| Face, arm, hand, and finger structure | No structural anomalies that impede language production |
| Gross and fine motor function | No impairments that impede language production |
| Physical and social interactions | No symptoms of impaired reciprocal social interaction or restriction of activities |
| Factor | Criteria |
|---|---|
| Language ability | Exposure to fluent signers at home and school beginning early in life. Sign language test scores of −1.25 SD or lower; at risk for social devalue |
| Nonverbal IQ | Performance IQ of 85 or higher |
| Vision | No impairment beyond corrected with glasses or contacts |
| Neurological dysfunction | No evidence of seizure disorders, cerebral palsy, brain lesions; not under medication for control of seizures |
| Face, arm, hand, and finger structure | No structural anomalies that impede language production |
| Gross and fine motor function | No impairments that impede language production |
| Physical and social interactions | No symptoms of impaired reciprocal social interaction or restriction of activities |
A further consideration for language screening is that signing deaf children can be considered developing bilinguals as they are not only acquiring a signed language (as a first language for native signers) but also a spoken language through its multiple modalities (i.e., spoken, written). There is considerable discussion in the literature on how signing deaf children in the US experience the English side of becoming ASL/English bilinguals. Whether English is a concurrent or sequential second language with early signing, deaf children differ in their access to and success with the multiple modalities of spoken language representation in their environment. Some rely more on speech, others use fingerspelling, signed English, the printed form, or some combination of forms. In different ways, each of these pathways for English acquisition may challenge our traditional frameworks for optimal literacy development. For example, do deaf readers rely on spoken phonology or do they use alternative sensory coding possibilities? Can they learn English directly through print? Does L1 competence transfer to L2 competence? See Goldin-Meadow & Mayberry (2001), Hoffmeister & Caldwell-Harris (2014), Mayberry, del Giudice, & Lieberman (2011), Mayer & Wells (1996) for examples of different facets of this discussion. Still, what we do know is that the majority of children who are born deaf, regardless of whether they speak or sign, struggle with English (Traxler, 2000). Yet, many studies suggest that the stronger one is in ASL, the stronger one is in English (Hoffmeister, Novogrodsky, Caldwell-Harris, Fish & Benedict, 2013; Hrastinsky & Wilbur, 2016; Israelite, Ewoldt, & Hoffmeister, 1992; Kyle & Harris, 2010; Mayberry, 2007; Padden & Hanson, 2000; Padden & Ramsey, 2000; Singleton, Morgan, DiGello, Wiles, & Rivers, 2004; Strong & Prinz, 1997, 2000). Mayberry (2007) summarizes a set of studies showing that high ASL proficient signers had an average of post-high school (i.e., secondary school) level reading scores, while low ASL proficient signers averaged third or fourth grade reading levels.
The purpose of this discussion is not to investigate whether the ASL/English link is causal or to make the case for an optimal model of ASL/English bilingualism development; rather, we seek simply to establish that ASL/English (bimodal) bilingualism is a normative linguistic experience for deaf children raised in signing families. We further recognize that while being a native signer of ASL typically ensures L1 ASL fluency, it does not “guarantee” successful English acquisition—English must be learned. Nevertheless, from the studies cited above, the odds favor that a native signing deaf child will demonstrate stronger English language outcomes than a deaf child who has weaker ASL skills. Thus, we would predict that if SLI were identified in an L1 native signer, they would also likely display language developmental delays in the various forms of their L2 (but see Woll & Morgan, 2012, for a counterexample to this prediction in the case of a child with Landau–Kleffner syndrome who was impaired in English but not in BSL).
One particularly interesting area of signed language structure with respect to language impairment is fingerspelling because it lies at the intersection of a signed and spoken/written language. Studies of deaf child and adult signers have established that ASL proficiency and fingerspelling skills are correlated (Emmorey & Petrich, 2012; Morere & Koo, 2012), thus we would expect a native ASL signer to demonstrate strong fingerspelling skills. Fingerspelling has also been shown to play a role in reading development for deaf signing children, and it has been suggested to provide links between English words and ASL signs (Crume, 2013; Humphries & MacDougall, 1999; Haptonstall-Nykaza & Schick, 2007; Padden 2006). As noted earlier, fingerspelling performance can also provide evidence of language deficit in deaf signing children (Marshall et al., 2015).
Such reports—appearing in the literature but often echoed by language professionals at schools for the deaf—provide the background for the suggestion that native ASL signers who exhibit pronounced reading challenges or fingerspelling difficulties would be seen as uncommon and would be particularly noticeable by educators and language specialists at schools for the Deaf.
This case study documents the profile of a deaf ASL–English bilingual with reported normal cognitive abilities, intact visual and motor abilities, but significant language developmental delays in ASL and English. This adolescent has a deaf father and a hearing mother, both of whom are signers of ASL. There were no environmental reasons for atypical language development because he was not deprived of linguistic input at school, and presumably the same is true for the home environment because his parents are fluent signers and his mother, in particular, was very involved as an advocate for this child. The aim of this study was to use mixed methods including interviews, review of documents, and neuropsychological and psychoeducational evaluations to describe the adolescent's strengths and weaknesses. The research questions that guided the study were the following: What is the profile of a deaf childhood signer of ASL with a proposed SLI? How does language impairment manifest in ASL and in English development? We hypothesized that there are cases of language impairment in the absence of general cognitive impairment within the population of deaf signing children, and SLI would be an appropriate diagnosis for such signed language users, based on modified diagnostic criteria. Additionally, it is hypothesized that aspects of both of a child's languages could be impacted, following similar reports for unimodal bilinguals (e.g., see Paradis, Crago, Genessee, & Rice, 2003; although, see Woll & Morgan, 2012 for a report that does not support this hypothesis).
Method
This study followed Quinto-Pozos, Singleton, Hauser & Levine's (2014) proposed method for investigating language impairment among deaf signing children. In this case, this approach involved multiple components and repeated visits with a deaf child at a school for the deaf in addition to interviews with adults familiar with the child over a period of 4 years. Interviews with parents, educators, and professionals at the school were combined with information from school records to gain an initial picture of the child's profile, which was then augmented with linguistic and cognitive data. A comprehensive neuropsychological evaluation was conducted to rule out other possible causes for the adolescent's reported language developmental delays. All research procedures were approved by the authors’ institutional review boards.
Participant
“Adam” is a native signing deaf child who was reported by his mother and school professionals to have difficulties with his ASL skill development despite being raised with the everyday use of ASL at home since birth and at school. Adam was exposed to parent and peer language models fluent in ASL throughout his childhood and adolescent years. Educational records documented that Adam exhibited atypical language development beyond expected of a student with his cognitive abilities that were reported in school psychological evaluations. The project team met with Adam multiple times during a period of 3.5 years when he was between the ages of 15;10 and 19;6. The visits would usually consist of Adam participating in conversation and semiformal language or cognitive tasks. Adam was also administered a full neuropsychological and psychoeducational evaluation during one particular visit (at age 17;11). Meetings usually occurred within 1 day, although multiple day visits, generally 1–2 hours per day, were also conducted to avoid test fatigue and excessive time away from classes. No information was collected about socioeconomic status of Adam's family, although we came to learn that his mother was very involved in his academic development. We note that Adam was in his last year of high school at our final visit (age 19;6); he did have academic difficulties that slowed his progress through the school years, which explains his relative older age than his high school senior peers.
Materials and Procedures
Sources of background information
Detailed medical, developmental, and educational history was obtained through interviews with Adam's mother, school professionals, and Adam. The interview with Adam's mother lasted slightly more than 1 hour, and discussions with the school professionals took between 15 and 30 minutes on two to three occasions. Two interviews with Adam (adult–child and child–peer) lasted between 15 and 45 minutes each. Questions were asked about Adam's strengths and weaknesses, his cognitive and language developmental history, and his educational history. Past records and documentation made during the time of this study were collected and analyzed including medical records, school psychology evaluations, speech and language evaluations, state standardized test results, and Individualized Education Program (IEP) Case Conference reports, documentation from formal assessments, informal assessments (e.g., developed by instructors or language specialists within the school), and extra services (e.g., information about intervention strategies and/or referrals for specific services such as speech language therapy or occupational therapy).
Neuropsychological and psychoeducational assessment
The neuropsychological assessment procedure utilized in this study followed the method proposed by Hauser, Quinto-Pozos, & Singleton (2015) for evaluating SLIs in deaf individuals. A battery of neuropsychological and psychoeducational assessments was used to examine Adam's general cognitive functioning, executive functioning, memory, motor skills, behavior and emotional functioning, visual processing, reading, and writing. A clinical neuropsychologist, who is deaf, administered all tests in ASL when Adam was 17;11. Only tests that are believed to be appropriate for deaf adolescents were administered: Wechsler Adult Intelligence Scale (Wechsler, 1997a); Test of Visual Perceptual Skills (TVPS) (Martin, 2006); Benton Facial Recognition Test (Benton, Hamsher, Varney, & Spreen, 1983); Grip Strength (Spreen & Strauss, 1998); Fingertapping Test (Spreen & Strauss, 1998); Grooved Pegboard (Baser & Ruff, 1987); Developmental Test of Visual Motor Integration (Berry & Beery, 2004); Color Trails Test (D'Elia, Satz, Uchiyama, & White, 1996); Wechsler Memory Scale (WMS) (Wechsler, 1997b); Rey–Osterrieth Complex Figure Test (Meyers & Meyers, 1995); Differential Abilities Scale (Elliot, 2007); and Brief Visual Memory Test (Benedict, 1997). The construct of each test and administrative procedures are described in Hauser et al., 2015.
ASL assessment
Signed language data for Adam were elicited using three primary tests: the American Sign Language–Sentence Reproduction Test (ASL-SRT, Hauser, Paludnevičiene, Supalla, & Bavelier, 2008; Supalla, Hauser, & Bavelier, 2014), the American Sign Language Proficiency Assessment (ASL-PA, Maller, Singleton, Supalla, & Wix, 1999), and the Fingerspelling Reproduction Test (Science of Learning Center on Visual Language and Visual Learning Toolkit, 2011). Details of each test are provided in Table 3.
Description of ASL Measures
| Test | Description and Procedures | Psychometric Information |
|---|---|---|
| American Sign Language–Sentence Reproduction Test | A 39-item measure of global ASL fluency including receptive, processing, and production skills; preliminary norms exist for children (beginning age 8 years) through adult age. Test takers are asked to repeat each sentence exactly as produced on the video display. Deviations from the original sentence (omissions, commissions, phonological errors, etc.) are scored as incorrect. Correct reproductions are awarded one point each item, and the maximum score for the test is 39. | High inter-rater reliability (R = .83) and internal consistency (alpha coefficient of 0.88; Hauser et al., 2008). |
| American Sign Language Proficiency Assessment | Using videorecordings of adult–child and child–peer interviews and a story-retelling as conversational and narrative source data, coders scrutinize a child's language production for the presence of 23 target structures across eight morpho-syntactic features of ASL (three examples of each feature are documented). ASL-PA scores reflect “overall general proficiency” and can be categorized into Low, Moderate, and High ASL Levels. It is not intended to provide diagnostic analysis of specific structure mastery. | Psychometric evaluation of the ASL-PA based on administration to 80 deaf ASL-using children between ages 6 and 12 years is reported in Maller, Singleton, Supalla, & Wix (1999). |
| Fingerspelling Reproduction Test | The test taker views 70 video clips of fingerspelled words (N = 45) and pseudo-words (N = 25) that were taken from the Spelling and Spelling of Sounds subtests of the Woodcock–Johnson III Tests of Achievement (Morere & Allen, 2012). The test items range from 2 to 13 letters in length (mean length = 6.18 letters). After viewing each video clip, the participant is required to repeat (i.e., fingerspell) the item they had just seen. A test taker's productions are scrutinized and scored for accuracy. | Based on a sample of 49 college-age students, young adults scored approximately 75% correct in total (raw score = 52.9/70; SD = 10.0), with similar performance for real and non–pseudo-words Morere & Koo (2012). Slightly higher performance (82% correct, SD = 18%) was obtained for a sample of 36 deaf signers (mean age = 28 years, 19 males) in a study by Emmorey & Petrich (2012). Performance on the Fingerspelling Test has been shown to correlate with ASL skill, as measured by the ASL-SRT (Emmorey & Petrich, 2012; Morere & Koo, 2012). |
| Test | Description and Procedures | Psychometric Information |
|---|---|---|
| American Sign Language–Sentence Reproduction Test | A 39-item measure of global ASL fluency including receptive, processing, and production skills; preliminary norms exist for children (beginning age 8 years) through adult age. Test takers are asked to repeat each sentence exactly as produced on the video display. Deviations from the original sentence (omissions, commissions, phonological errors, etc.) are scored as incorrect. Correct reproductions are awarded one point each item, and the maximum score for the test is 39. | High inter-rater reliability (R = .83) and internal consistency (alpha coefficient of 0.88; Hauser et al., 2008). |
| American Sign Language Proficiency Assessment | Using videorecordings of adult–child and child–peer interviews and a story-retelling as conversational and narrative source data, coders scrutinize a child's language production for the presence of 23 target structures across eight morpho-syntactic features of ASL (three examples of each feature are documented). ASL-PA scores reflect “overall general proficiency” and can be categorized into Low, Moderate, and High ASL Levels. It is not intended to provide diagnostic analysis of specific structure mastery. | Psychometric evaluation of the ASL-PA based on administration to 80 deaf ASL-using children between ages 6 and 12 years is reported in Maller, Singleton, Supalla, & Wix (1999). |
| Fingerspelling Reproduction Test | The test taker views 70 video clips of fingerspelled words (N = 45) and pseudo-words (N = 25) that were taken from the Spelling and Spelling of Sounds subtests of the Woodcock–Johnson III Tests of Achievement (Morere & Allen, 2012). The test items range from 2 to 13 letters in length (mean length = 6.18 letters). After viewing each video clip, the participant is required to repeat (i.e., fingerspell) the item they had just seen. A test taker's productions are scrutinized and scored for accuracy. | Based on a sample of 49 college-age students, young adults scored approximately 75% correct in total (raw score = 52.9/70; SD = 10.0), with similar performance for real and non–pseudo-words Morere & Koo (2012). Slightly higher performance (82% correct, SD = 18%) was obtained for a sample of 36 deaf signers (mean age = 28 years, 19 males) in a study by Emmorey & Petrich (2012). Performance on the Fingerspelling Test has been shown to correlate with ASL skill, as measured by the ASL-SRT (Emmorey & Petrich, 2012; Morere & Koo, 2012). |
Description of ASL Measures
| Test | Description and Procedures | Psychometric Information |
|---|---|---|
| American Sign Language–Sentence Reproduction Test | A 39-item measure of global ASL fluency including receptive, processing, and production skills; preliminary norms exist for children (beginning age 8 years) through adult age. Test takers are asked to repeat each sentence exactly as produced on the video display. Deviations from the original sentence (omissions, commissions, phonological errors, etc.) are scored as incorrect. Correct reproductions are awarded one point each item, and the maximum score for the test is 39. | High inter-rater reliability (R = .83) and internal consistency (alpha coefficient of 0.88; Hauser et al., 2008). |
| American Sign Language Proficiency Assessment | Using videorecordings of adult–child and child–peer interviews and a story-retelling as conversational and narrative source data, coders scrutinize a child's language production for the presence of 23 target structures across eight morpho-syntactic features of ASL (three examples of each feature are documented). ASL-PA scores reflect “overall general proficiency” and can be categorized into Low, Moderate, and High ASL Levels. It is not intended to provide diagnostic analysis of specific structure mastery. | Psychometric evaluation of the ASL-PA based on administration to 80 deaf ASL-using children between ages 6 and 12 years is reported in Maller, Singleton, Supalla, & Wix (1999). |
| Fingerspelling Reproduction Test | The test taker views 70 video clips of fingerspelled words (N = 45) and pseudo-words (N = 25) that were taken from the Spelling and Spelling of Sounds subtests of the Woodcock–Johnson III Tests of Achievement (Morere & Allen, 2012). The test items range from 2 to 13 letters in length (mean length = 6.18 letters). After viewing each video clip, the participant is required to repeat (i.e., fingerspell) the item they had just seen. A test taker's productions are scrutinized and scored for accuracy. | Based on a sample of 49 college-age students, young adults scored approximately 75% correct in total (raw score = 52.9/70; SD = 10.0), with similar performance for real and non–pseudo-words Morere & Koo (2012). Slightly higher performance (82% correct, SD = 18%) was obtained for a sample of 36 deaf signers (mean age = 28 years, 19 males) in a study by Emmorey & Petrich (2012). Performance on the Fingerspelling Test has been shown to correlate with ASL skill, as measured by the ASL-SRT (Emmorey & Petrich, 2012; Morere & Koo, 2012). |
| Test | Description and Procedures | Psychometric Information |
|---|---|---|
| American Sign Language–Sentence Reproduction Test | A 39-item measure of global ASL fluency including receptive, processing, and production skills; preliminary norms exist for children (beginning age 8 years) through adult age. Test takers are asked to repeat each sentence exactly as produced on the video display. Deviations from the original sentence (omissions, commissions, phonological errors, etc.) are scored as incorrect. Correct reproductions are awarded one point each item, and the maximum score for the test is 39. | High inter-rater reliability (R = .83) and internal consistency (alpha coefficient of 0.88; Hauser et al., 2008). |
| American Sign Language Proficiency Assessment | Using videorecordings of adult–child and child–peer interviews and a story-retelling as conversational and narrative source data, coders scrutinize a child's language production for the presence of 23 target structures across eight morpho-syntactic features of ASL (three examples of each feature are documented). ASL-PA scores reflect “overall general proficiency” and can be categorized into Low, Moderate, and High ASL Levels. It is not intended to provide diagnostic analysis of specific structure mastery. | Psychometric evaluation of the ASL-PA based on administration to 80 deaf ASL-using children between ages 6 and 12 years is reported in Maller, Singleton, Supalla, & Wix (1999). |
| Fingerspelling Reproduction Test | The test taker views 70 video clips of fingerspelled words (N = 45) and pseudo-words (N = 25) that were taken from the Spelling and Spelling of Sounds subtests of the Woodcock–Johnson III Tests of Achievement (Morere & Allen, 2012). The test items range from 2 to 13 letters in length (mean length = 6.18 letters). After viewing each video clip, the participant is required to repeat (i.e., fingerspell) the item they had just seen. A test taker's productions are scrutinized and scored for accuracy. | Based on a sample of 49 college-age students, young adults scored approximately 75% correct in total (raw score = 52.9/70; SD = 10.0), with similar performance for real and non–pseudo-words Morere & Koo (2012). Slightly higher performance (82% correct, SD = 18%) was obtained for a sample of 36 deaf signers (mean age = 28 years, 19 males) in a study by Emmorey & Petrich (2012). Performance on the Fingerspelling Test has been shown to correlate with ASL skill, as measured by the ASL-SRT (Emmorey & Petrich, 2012; Morere & Koo, 2012). |
Adam completed the original 39-item version of the ASL-SRT on three different occasions: when he was 17;11, 18;11, and 19;6. Repetition of the test over multiple years allowed for the tracking of performance changes over time. The ASL-PA was administered during the first meeting with Adam, which took place when he was age 15;10. This test was administered even though the suggested age range is 6–12 years because it is not uncommon for children with language impairment to perform like younger users of a language. The first two parts of the ASL-PA were administered in that first data collection session: the adult–child interview and the child retelling of the Tortoise and the Hare story in ASL. The third part (child–peer interview) was completed when Adam was 16 years old. The adults were: (1) a hearing researcher who is a linguist and a certified ASL–English interpreter and (2) a hearing developmental psychologist and native signer of ASL. The peer was one of Adam's friends who was a non-native signer who had moved from another country to the US after age 7 years. Adam was given his choice of conversational partner to encourage a casual dialogue/conversation between the two in hopes of generating as much language use as possible by Adam.
The Fingerspelling Reproduction Test was administered when Adam was 17;11 and then again at 18;11. An additional measure of fingerspelling was created for this project in which many of the real-word fingerspelled items from The Fingerspelling Reproduction Test are embedded in an ASL narrative, and then the test taker is queried about the meaning of the fingerspelled items; this measure was administered when Adam was 19;6. This approach allows for the embedding of fingerspelled items within natural ASL discourse, rather than simply appearing as tokens of fingerspelling in isolation. For this task, the test taker views the entire narrative (presented in prerecorded ASL by a native deaf signer), and then the video is replayed, this time with the test administrator pausing after each phrase and querying the test taker about the fingerspelled word that appeared in that segment. Test takers are questioned about what the fingerspelled word means, and they are asked to respond in ASL. This approach allows for the examination of a test taker's processing of fingerspelled items and also the extent to which the test taker is able to predict the meaning from context. See Appendix A for the narrative that was created with the fingerspelled items.
English assessment
Adam's scores on English assessments in his educational records were collected. This included the results of his performance on the Stanford Achievement Test (Harcourt Educational Measurement, 1996), which provide both hearing and deaf normative data. Past performance on the following tests were also collected: Trophies Placement and Diagnostic Assessment (Trophies, 2003); Woodcock–Johnson Tests of Achievement (Woodcock, McGrew, & Mather, 2001); and Oral and Written Language Scales (Carrow-Woolfolk, 1995). Adam's scores on his state's standardized educational tests were also documented—the name of the state is omitted here to protect Adam's confidentiality. During the neuropsychological evaluation, a psychoeducational evaluation was also conducted with the Woodcock–Johnson Test of Achievement to obtain qualitative data on his test performance and responses as well as his quantitative test scores.
Results
Background Information
Adam's neonatal, perinatal, and birth history were unremarkable, and he achieved early developmental milestones at appropriate times with the exception of language development. Adam's mother reported that his expressive and receptive language development was delayed in early life. She and school personnel first noticed this when Adam was 3 years old. The observed delayed language development continued throughout his early years, and his mother reported that in the beginning, school professionals believed that he was just a ‘late bloomer’ perhaps because his physical and social skills were normal. He had multiple friends and he participated in social activities. As an adolescent, he played on the school's competitive sports teams.
Adam's mother also mentioned how he can generally follow conversations in ASL “…as long as there is no fingerspelling.” Similarly, school professionals indicated multiple times that Adam exhibited particular difficulty with ASL fingerspelling reception, along with isolated examples of other challenges. Adam's English literacy skills were also notably impaired throughout his school years on standardized tests. His mother noted, “We also see spelling problems in (English) writing and fingerspelling. (He is) …definitively behind in writing and reading and they just can't seem to give a reason why or figure out why he has the problems.”
Adam was given individualized attention regarding his signed language development at school. He received one-on-one tutoring, attended occupational therapy sessions, and received speech and language intervention services. These intervention efforts may have had a positive impact, and his ASL skills were reported to have improved slowly over time. Adam received some tutoring in ASL by language specialists, and some of the linguistic devices that were covered in tutoring sessions included: questions, facial expressions, and setting up a narrative framework (e.g., a beginning, middle, and end to a story).
Adam was also diagnosed with attention-deficit hyperactivity disorder (ADHD) during his early elementary years and took medication to treat the ADHD. He also has a history of having a mild tic disorder. However, in recent years, Adam's school psychologist and other school personnel believed that his language difficulties were beyond what would be expected of a child with ADHD and a tic disorder, although it is possible that these disorders, if accurately diagnosed, exacerbated his language difficulties.
Assessment of Neuropsychological Functioning
Adam had been administered various standardized tests of cognition and language over his school years, and at least two reports from school psychologists (ages 12;8 and 14;4) reported that Adam's nonverbal intelligence was within the average range, and some of his subtest scores were within the high average range. The results of the neuropsychological evaluation performed for this study confirmed the earlier reports of his intellectual ability (Table 4). Consistent with previous testing, Adam's overall visual perceptual skills, facial recognition abilities, and gross and fine motor skills were within the average range.
Results of Neuropsychological Evaluation (Adam 17;11)
| Domain | Test | Score | Range |
|---|---|---|---|
| Intelligence | Wechsler Adult Intelligence Scale (WAIS) | Performance IQ SS = 92 | Average |
| Perceptual Organization Index SS = 95 | Average | ||
| Processing Speed Index SS = 106 | Average | ||
| Picture Completion Subscale Score = 9 | Average | ||
| Digit Symbol Subscale Score = 10 | Average | ||
| Block Design Subscale Score = 13 | Average | ||
| Matrix Reasoning Subscale Score = 6 | Low Average | ||
| Digit Span Subscale Score = 5 | Impaired | ||
| Picture Arrangement Subscale Score = 7 | Average | ||
| Symbol Search Subscale Score = 12 | Average | ||
| Vision | |||
| Visual Perception | Test of Visual Perceptual Skills-3 (TVPS) | Visual Perceptual Quotient SS = 98 | Average |
| Basic Processes SS = 96 | Average | ||
| Sequencing SS = 75 | Low Average | ||
| Complex Processes SS = 105 | Average | ||
| Visual Discrimination Scaled Score = 12 | Average | ||
| Visual Memory Scaled Score = 9 | Average | ||
| Spatial Relations Scaled Score = 8 | Average | ||
| Form Constancy Scaled Score = 8 | Average | ||
| Sequential Memory Scaled Score = 5 | Impaired | ||
| Figure Ground Scaled Score = 9 | Average | ||
| Visual Closure Scaled Score = 13 | Average | ||
| Facial | Benton Facial | Raw Score = 44 | WNL |
| Recognition | Recognition Test | ||
| Motor Skills | |||
| Gross Motor | Grip Strength | Dominant Hand = 49.6 kg | WNL |
| Non-dominant Hand = 54.3 kg | WNL | ||
| Fine Motor | Fingertapping Test | Dominant Hand = 54 taps | WNL |
| Non-dominant Hand = 44 taps | WNL | ||
| Visual Motor Coordination | Grooved Pegboard | Dominant Hand = 54.4 Sec. | WNL |
| Non-dominant Hand = 62.4 Sec. | WNL | ||
| Visual Motor Integration | Developmental Test of Visual Motor Integration | SS = 95 | Average |
| Attention | |||
| WAIS Coding Subtest | Scaled Score = 10 | Average | |
| WAIS Symbol Search | Scaled Score = 12 | Average | |
| Executive Function | |||
| Color Trails Test | Trail 1 SS = 125 | Above Average | |
| Trail 2 SS = 102 | Average | ||
| Memory | |||
| Visual Short-Term Memory | TVPS Visual Memory | Scaled Score = 9 | Average |
| Spatial Short-Term Memory | Weschler Memory Scale Spatial Span | Scaled Score = 11 | Average |
| Visual Working Memory | Mental Rotation Test | Raw Score = 14 | Average |
| Immediate and Delayed Memory | Rey–Osterrieth Complex Figure Test | Immediate Recall T-Score = 26 | Impaired |
| Delayed Recall T-Score = 36 | Low Average | ||
| Differential Abilities Scale Recall of Objects | Immediate Recall T-Score = 27 | Impaired | |
| Delayed Recall T-Score = 37 | Low Average | ||
| Brief Visual Memory Test | Immediate Recall T-Score = 28 | Impaired | |
| Delayed Recall T-Score = 44 | Average | ||
| Domain | Test | Score | Range |
|---|---|---|---|
| Intelligence | Wechsler Adult Intelligence Scale (WAIS) | Performance IQ SS = 92 | Average |
| Perceptual Organization Index SS = 95 | Average | ||
| Processing Speed Index SS = 106 | Average | ||
| Picture Completion Subscale Score = 9 | Average | ||
| Digit Symbol Subscale Score = 10 | Average | ||
| Block Design Subscale Score = 13 | Average | ||
| Matrix Reasoning Subscale Score = 6 | Low Average | ||
| Digit Span Subscale Score = 5 | Impaired | ||
| Picture Arrangement Subscale Score = 7 | Average | ||
| Symbol Search Subscale Score = 12 | Average | ||
| Vision | |||
| Visual Perception | Test of Visual Perceptual Skills-3 (TVPS) | Visual Perceptual Quotient SS = 98 | Average |
| Basic Processes SS = 96 | Average | ||
| Sequencing SS = 75 | Low Average | ||
| Complex Processes SS = 105 | Average | ||
| Visual Discrimination Scaled Score = 12 | Average | ||
| Visual Memory Scaled Score = 9 | Average | ||
| Spatial Relations Scaled Score = 8 | Average | ||
| Form Constancy Scaled Score = 8 | Average | ||
| Sequential Memory Scaled Score = 5 | Impaired | ||
| Figure Ground Scaled Score = 9 | Average | ||
| Visual Closure Scaled Score = 13 | Average | ||
| Facial | Benton Facial | Raw Score = 44 | WNL |
| Recognition | Recognition Test | ||
| Motor Skills | |||
| Gross Motor | Grip Strength | Dominant Hand = 49.6 kg | WNL |
| Non-dominant Hand = 54.3 kg | WNL | ||
| Fine Motor | Fingertapping Test | Dominant Hand = 54 taps | WNL |
| Non-dominant Hand = 44 taps | WNL | ||
| Visual Motor Coordination | Grooved Pegboard | Dominant Hand = 54.4 Sec. | WNL |
| Non-dominant Hand = 62.4 Sec. | WNL | ||
| Visual Motor Integration | Developmental Test of Visual Motor Integration | SS = 95 | Average |
| Attention | |||
| WAIS Coding Subtest | Scaled Score = 10 | Average | |
| WAIS Symbol Search | Scaled Score = 12 | Average | |
| Executive Function | |||
| Color Trails Test | Trail 1 SS = 125 | Above Average | |
| Trail 2 SS = 102 | Average | ||
| Memory | |||
| Visual Short-Term Memory | TVPS Visual Memory | Scaled Score = 9 | Average |
| Spatial Short-Term Memory | Weschler Memory Scale Spatial Span | Scaled Score = 11 | Average |
| Visual Working Memory | Mental Rotation Test | Raw Score = 14 | Average |
| Immediate and Delayed Memory | Rey–Osterrieth Complex Figure Test | Immediate Recall T-Score = 26 | Impaired |
| Delayed Recall T-Score = 36 | Low Average | ||
| Differential Abilities Scale Recall of Objects | Immediate Recall T-Score = 27 | Impaired | |
| Delayed Recall T-Score = 37 | Low Average | ||
| Brief Visual Memory Test | Immediate Recall T-Score = 28 | Impaired | |
| Delayed Recall T-Score = 44 | Average | ||
Note: Wechsler Adult Intelligence Scale was used because Adam was close to the age of 18 years at the time of testing. He is right-handed. WNL = Within Normal limits; SS = Standard Scores (M= 100; SD = 15). T-scores have M of 50, SD of 10 and Scaled Scores have M of 10 and SD of 3. Scores that were between–1 and–1.5 SD are termed here as “Low Average,” between –1.5 and –2 SD as “Below Average,” and more than –2 SD as “Impaired.”
Results of Neuropsychological Evaluation (Adam 17;11)
| Domain | Test | Score | Range |
|---|---|---|---|
| Intelligence | Wechsler Adult Intelligence Scale (WAIS) | Performance IQ SS = 92 | Average |
| Perceptual Organization Index SS = 95 | Average | ||
| Processing Speed Index SS = 106 | Average | ||
| Picture Completion Subscale Score = 9 | Average | ||
| Digit Symbol Subscale Score = 10 | Average | ||
| Block Design Subscale Score = 13 | Average | ||
| Matrix Reasoning Subscale Score = 6 | Low Average | ||
| Digit Span Subscale Score = 5 | Impaired | ||
| Picture Arrangement Subscale Score = 7 | Average | ||
| Symbol Search Subscale Score = 12 | Average | ||
| Vision | |||
| Visual Perception | Test of Visual Perceptual Skills-3 (TVPS) | Visual Perceptual Quotient SS = 98 | Average |
| Basic Processes SS = 96 | Average | ||
| Sequencing SS = 75 | Low Average | ||
| Complex Processes SS = 105 | Average | ||
| Visual Discrimination Scaled Score = 12 | Average | ||
| Visual Memory Scaled Score = 9 | Average | ||
| Spatial Relations Scaled Score = 8 | Average | ||
| Form Constancy Scaled Score = 8 | Average | ||
| Sequential Memory Scaled Score = 5 | Impaired | ||
| Figure Ground Scaled Score = 9 | Average | ||
| Visual Closure Scaled Score = 13 | Average | ||
| Facial | Benton Facial | Raw Score = 44 | WNL |
| Recognition | Recognition Test | ||
| Motor Skills | |||
| Gross Motor | Grip Strength | Dominant Hand = 49.6 kg | WNL |
| Non-dominant Hand = 54.3 kg | WNL | ||
| Fine Motor | Fingertapping Test | Dominant Hand = 54 taps | WNL |
| Non-dominant Hand = 44 taps | WNL | ||
| Visual Motor Coordination | Grooved Pegboard | Dominant Hand = 54.4 Sec. | WNL |
| Non-dominant Hand = 62.4 Sec. | WNL | ||
| Visual Motor Integration | Developmental Test of Visual Motor Integration | SS = 95 | Average |
| Attention | |||
| WAIS Coding Subtest | Scaled Score = 10 | Average | |
| WAIS Symbol Search | Scaled Score = 12 | Average | |
| Executive Function | |||
| Color Trails Test | Trail 1 SS = 125 | Above Average | |
| Trail 2 SS = 102 | Average | ||
| Memory | |||
| Visual Short-Term Memory | TVPS Visual Memory | Scaled Score = 9 | Average |
| Spatial Short-Term Memory | Weschler Memory Scale Spatial Span | Scaled Score = 11 | Average |
| Visual Working Memory | Mental Rotation Test | Raw Score = 14 | Average |
| Immediate and Delayed Memory | Rey–Osterrieth Complex Figure Test | Immediate Recall T-Score = 26 | Impaired |
| Delayed Recall T-Score = 36 | Low Average | ||
| Differential Abilities Scale Recall of Objects | Immediate Recall T-Score = 27 | Impaired | |
| Delayed Recall T-Score = 37 | Low Average | ||
| Brief Visual Memory Test | Immediate Recall T-Score = 28 | Impaired | |
| Delayed Recall T-Score = 44 | Average | ||
| Domain | Test | Score | Range |
|---|---|---|---|
| Intelligence | Wechsler Adult Intelligence Scale (WAIS) | Performance IQ SS = 92 | Average |
| Perceptual Organization Index SS = 95 | Average | ||
| Processing Speed Index SS = 106 | Average | ||
| Picture Completion Subscale Score = 9 | Average | ||
| Digit Symbol Subscale Score = 10 | Average | ||
| Block Design Subscale Score = 13 | Average | ||
| Matrix Reasoning Subscale Score = 6 | Low Average | ||
| Digit Span Subscale Score = 5 | Impaired | ||
| Picture Arrangement Subscale Score = 7 | Average | ||
| Symbol Search Subscale Score = 12 | Average | ||
| Vision | |||
| Visual Perception | Test of Visual Perceptual Skills-3 (TVPS) | Visual Perceptual Quotient SS = 98 | Average |
| Basic Processes SS = 96 | Average | ||
| Sequencing SS = 75 | Low Average | ||
| Complex Processes SS = 105 | Average | ||
| Visual Discrimination Scaled Score = 12 | Average | ||
| Visual Memory Scaled Score = 9 | Average | ||
| Spatial Relations Scaled Score = 8 | Average | ||
| Form Constancy Scaled Score = 8 | Average | ||
| Sequential Memory Scaled Score = 5 | Impaired | ||
| Figure Ground Scaled Score = 9 | Average | ||
| Visual Closure Scaled Score = 13 | Average | ||
| Facial | Benton Facial | Raw Score = 44 | WNL |
| Recognition | Recognition Test | ||
| Motor Skills | |||
| Gross Motor | Grip Strength | Dominant Hand = 49.6 kg | WNL |
| Non-dominant Hand = 54.3 kg | WNL | ||
| Fine Motor | Fingertapping Test | Dominant Hand = 54 taps | WNL |
| Non-dominant Hand = 44 taps | WNL | ||
| Visual Motor Coordination | Grooved Pegboard | Dominant Hand = 54.4 Sec. | WNL |
| Non-dominant Hand = 62.4 Sec. | WNL | ||
| Visual Motor Integration | Developmental Test of Visual Motor Integration | SS = 95 | Average |
| Attention | |||
| WAIS Coding Subtest | Scaled Score = 10 | Average | |
| WAIS Symbol Search | Scaled Score = 12 | Average | |
| Executive Function | |||
| Color Trails Test | Trail 1 SS = 125 | Above Average | |
| Trail 2 SS = 102 | Average | ||
| Memory | |||
| Visual Short-Term Memory | TVPS Visual Memory | Scaled Score = 9 | Average |
| Spatial Short-Term Memory | Weschler Memory Scale Spatial Span | Scaled Score = 11 | Average |
| Visual Working Memory | Mental Rotation Test | Raw Score = 14 | Average |
| Immediate and Delayed Memory | Rey–Osterrieth Complex Figure Test | Immediate Recall T-Score = 26 | Impaired |
| Delayed Recall T-Score = 36 | Low Average | ||
| Differential Abilities Scale Recall of Objects | Immediate Recall T-Score = 27 | Impaired | |
| Delayed Recall T-Score = 37 | Low Average | ||
| Brief Visual Memory Test | Immediate Recall T-Score = 28 | Impaired | |
| Delayed Recall T-Score = 44 | Average | ||
Note: Wechsler Adult Intelligence Scale was used because Adam was close to the age of 18 years at the time of testing. He is right-handed. WNL = Within Normal limits; SS = Standard Scores (M= 100; SD = 15). T-scores have M of 50, SD of 10 and Scaled Scores have M of 10 and SD of 3. Scores that were between–1 and–1.5 SD are termed here as “Low Average,” between –1.5 and –2 SD as “Below Average,” and more than –2 SD as “Impaired.”
In contrast to results obtained from tests of general intelligence, visual–spatial skills, and motor skills, Adam had marked difficulties with memory and sequential processing. He scored in the Impaired range (2SD below the mean) on various tests that involve memory and/or sequencing including: (a) Wechsler Adult Intelligence Scale Digit Span Subtest; (b) TVPS Sequencing Subscale; (c) Rey–Osterrieth Complex Figure Test Immediate Recall; (d) Differential Abilities Scale Recall of Objects test; and (e) Brief Visual Memory Test Immediate Recall. Adam also performed within the Low Average range (between −1 SD and −1.5SD below the mean, according to the criteria we are following) on several tests: (a) Wechsler Adult Intelligence Scale Matrix Reasoning Subscale; (b) TVPS Sequencing Subtest; (c) Rey–Osterrieth Complex Figure Test Delay Recall; and (d) Differential Abilities Scale Recall of Objects Subtest.
Regarding Adam's prior diagnosis of ADHD, the authors noted that on several occasions, data collection sessions with Adam sometimes lasted for multiple hours, and there were no obvious signs of attentional issues; in fact, Adam exhibited excellent attention and patience throughout. He performed in the average range on tests that are sensitive to attentional difficulties (e.g., Weschler Adult Intelligence Scale Processing Speed Index, Symbol Search Subtest, Digit Symbol Subtest, and Coding Subtest; WMS Spatial Span Subtest). The results support observation that he was able to stay very focused during testing sessions. It is possible that the observed ADHD symptoms by his family and school were better explained by memory and sequential difficulties or that Adam's medication was supporting maintained attention during those sessions. Another possibility is that Adam was misdiagnosed earlier in his childhood. We did not pursue this further because of his high level of attention during our sessions. In addition, with his reported language delays, he might have appeared restless or unclear of what is going on at times causing inattentive and hyperactive behaviors. Regardless, if Adam has attentional issues, they are not significant enough to explain his reported language developmental delays.
Assessment of ASL Skills
AST-SRT
Adam has marked difficulty with his global receptive and expressive ASL fluency as measured by the ASL-SRT over a period of 3 years (Table 5). Adam's performance was well below what would be expected of an adult native signer (−3 SD below the adult mean on the first two administrations) and a child native signer (−2 to −3 SD below) based on the norms for native signers that are reported in Hauser et al. (2008). Adam's performance improved modestly from the first to the third administrations although he remained significantly below the 1.25 SD that serves as the cutoff for language impairment as suggested in the diagnostic criteria for SLI (Leonard, 1998).
Adam's Performance on the ASL-SRT Compared to Other Native Signers
| Adam's Age (years; months) | Score | Native Signing Children Scores (n = 27; Mage = 12.5, SD = 1.5) | Native Signing Adults Scores (n = 23; Mage = 23.4, SD = 4.4) |
|---|---|---|---|
| 17;11 | 5 | 23.9 (4.4) | 25.9 (4.3) |
| 18;11 | 7 | ||
| 19;6 | 13 |
| Adam's Age (years; months) | Score | Native Signing Children Scores (n = 27; Mage = 12.5, SD = 1.5) | Native Signing Adults Scores (n = 23; Mage = 23.4, SD = 4.4) |
|---|---|---|---|
| 17;11 | 5 | 23.9 (4.4) | 25.9 (4.3) |
| 18;11 | 7 | ||
| 19;6 | 13 |
Note: Raw scores reported using Mean and SD.
Adam's Performance on the ASL-SRT Compared to Other Native Signers
| Adam's Age (years; months) | Score | Native Signing Children Scores (n = 27; Mage = 12.5, SD = 1.5) | Native Signing Adults Scores (n = 23; Mage = 23.4, SD = 4.4) |
|---|---|---|---|
| 17;11 | 5 | 23.9 (4.4) | 25.9 (4.3) |
| 18;11 | 7 | ||
| 19;6 | 13 |
| Adam's Age (years; months) | Score | Native Signing Children Scores (n = 27; Mage = 12.5, SD = 1.5) | Native Signing Adults Scores (n = 23; Mage = 23.4, SD = 4.4) |
|---|---|---|---|
| 17;11 | 5 | 23.9 (4.4) | 25.9 (4.3) |
| 18;11 | 7 | ||
| 19;6 | 13 |
Note: Raw scores reported using Mean and SD.
Qualitative analysis of Adam's reproductions of the ASL-SRT sentences illustrates how his ASL skills improved over a period of 3 years. On the first administration, he frequently omitted signs or added signs that were not in the target sentence. There were also issues with reproducing the word order of some sentences. Such errors decreased somewhat on the second and third administrations of the test—with the final set of responses containing more of the target signs and sentence structures. However, within all three administrations of the ASL-SRT, longer and more complex sentences to-be-remembered were particularly challenging for Adam. On all test administrations, he immediately became flustered when encountering fingerspelled items and subsequently struggled to reproduce the overall sentence. He was only able to reproduce one fingerspelled item that had a common lexicalized form (#BANK).
ASL-PA
Adam's performance on the ASL-PA illustrated that he is able to carry on a conversation in ASL with his interlocutors (both with adults and with his age- and gender-matched peer). Adam's comprehension skills appeared typical, he remembered all components of the presented cartoon for retelling, and his ability to respond to a majority of the questions posed to him was generally quite good. With respect to his ASL-PA performance score (using the scoring rubric developed by Maller et al., 1999), Adam demonstrated 22 of the 23 target linguistic structures successfully. A score of 22 on the ASL-PA puts Adam in the Level 3 (Highest Proficiency) category (which is 17 and higher, using cutoffs drawn from a psychometric analysis of a sample of 80 deaf signing 6–12 year olds, Maller et al., 1999). We note that fingerspelling is not one of the target structures for scoring on the ASL-PA.
Adam's only missing ASL-PA target structure (out of 23) was Real-World Location Verb Agreement Marking. This gap is not uncommon on the ASL-PA because there often is no context in the three discourse categories that elicit a point-to-real-world location. However, Adam did successfully produce abstract verb agreement (the use of a locus in the signing space that represents the argument noun phrase of the verb), which strongly suggests that he would be able to do real-world verb agreement. While the ASL-PA is not designed to be a diagnostic tool, it does provide a kind of omnibus classification of High, Moderate, or Low ASL proficiency, without the consideration of fingerspelling. One can also do well on the ASL-PA with short conversational turns that are grammatical and do not tax sequential memory.
Because of his known difficulty with fingerspelling, we conducted an analysis of Adam's fingerspelling use during the conversational sessions that comprised the ASL-PA data collection. Adam's performance was compared with that of his peer participating in the same conversation. The broad categories used for analysis were: lexicalized fingerspelling (e.g., those items that are most sign-like like #BACK), proper nouns (e.g., K-E-N), and common nouns (e.g., P-U-P-P-Y). In addition, if a signer articulated a fingerspelled word that was not clearly produced and/or contained a semantic intent that was not clear from context, that item was coded as “unsure.” See Table 6 for the categorization of lexical items from the ASL-PA sessions.
Fingerspelling by All Interlocutors in the ASL-PA Data Collection Sessions
| Total No. of Words | Total No. of Unique Words | Lexicalized (i.e., “Loan Sign”) | Non-Lexicalized; Proper Noun | Non-Lexicalized, Common Noun | Unsure | |
|---|---|---|---|---|---|---|
| Session with adults (33 minutes) | ||||||
| Adam (15;10) | 52 | 33 (63.5%) | 20 (38.4%) | 23 (44.2%) | 9 (17.3%) | 4 (7.7%) |
| Adult 1 | 55 | 28 (51%) | 43 (78%) | 2 (3.6%) | 10 (18.1%) | 1 (1.9%) |
| Adult 2 | 38 | 22 (57.9%) | 19 (50%) | 13 (34.2%) | 6 (15.8%) | - |
| Session with peer (15 minutes) | ||||||
| Adam | 34 | 26 (76.4%) | 20 (58.8%) | 6 (17.6%) | 8 (23.5%) | 1 (2.9%) |
| Peer | 59 | 35 (59.3%) | 29 (49.1%) | 23 (40%) | 7 (11.9%) | - |
| Total No. of Words | Total No. of Unique Words | Lexicalized (i.e., “Loan Sign”) | Non-Lexicalized; Proper Noun | Non-Lexicalized, Common Noun | Unsure | |
|---|---|---|---|---|---|---|
| Session with adults (33 minutes) | ||||||
| Adam (15;10) | 52 | 33 (63.5%) | 20 (38.4%) | 23 (44.2%) | 9 (17.3%) | 4 (7.7%) |
| Adult 1 | 55 | 28 (51%) | 43 (78%) | 2 (3.6%) | 10 (18.1%) | 1 (1.9%) |
| Adult 2 | 38 | 22 (57.9%) | 19 (50%) | 13 (34.2%) | 6 (15.8%) | - |
| Session with peer (15 minutes) | ||||||
| Adam | 34 | 26 (76.4%) | 20 (58.8%) | 6 (17.6%) | 8 (23.5%) | 1 (2.9%) |
| Peer | 59 | 35 (59.3%) | 29 (49.1%) | 23 (40%) | 7 (11.9%) | - |
Fingerspelling by All Interlocutors in the ASL-PA Data Collection Sessions
| Total No. of Words | Total No. of Unique Words | Lexicalized (i.e., “Loan Sign”) | Non-Lexicalized; Proper Noun | Non-Lexicalized, Common Noun | Unsure | |
|---|---|---|---|---|---|---|
| Session with adults (33 minutes) | ||||||
| Adam (15;10) | 52 | 33 (63.5%) | 20 (38.4%) | 23 (44.2%) | 9 (17.3%) | 4 (7.7%) |
| Adult 1 | 55 | 28 (51%) | 43 (78%) | 2 (3.6%) | 10 (18.1%) | 1 (1.9%) |
| Adult 2 | 38 | 22 (57.9%) | 19 (50%) | 13 (34.2%) | 6 (15.8%) | - |
| Session with peer (15 minutes) | ||||||
| Adam | 34 | 26 (76.4%) | 20 (58.8%) | 6 (17.6%) | 8 (23.5%) | 1 (2.9%) |
| Peer | 59 | 35 (59.3%) | 29 (49.1%) | 23 (40%) | 7 (11.9%) | - |
| Total No. of Words | Total No. of Unique Words | Lexicalized (i.e., “Loan Sign”) | Non-Lexicalized; Proper Noun | Non-Lexicalized, Common Noun | Unsure | |
|---|---|---|---|---|---|---|
| Session with adults (33 minutes) | ||||||
| Adam (15;10) | 52 | 33 (63.5%) | 20 (38.4%) | 23 (44.2%) | 9 (17.3%) | 4 (7.7%) |
| Adult 1 | 55 | 28 (51%) | 43 (78%) | 2 (3.6%) | 10 (18.1%) | 1 (1.9%) |
| Adult 2 | 38 | 22 (57.9%) | 19 (50%) | 13 (34.2%) | 6 (15.8%) | - |
| Session with peer (15 minutes) | ||||||
| Adam | 34 | 26 (76.4%) | 20 (58.8%) | 6 (17.6%) | 8 (23.5%) | 1 (2.9%) |
| Peer | 59 | 35 (59.3%) | 29 (49.1%) | 23 (40%) | 7 (11.9%) | - |
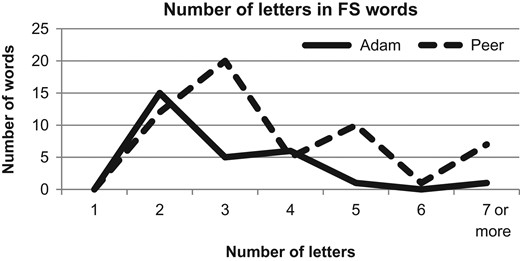
Lengths of fingerspelled items for the ASL-PA peer interaction.
Fingerspelling Reproduction Test
Adam's fingerspelling difficulties were evident on the Fingerspelling Reproduction Test at 17;11, and then again at 18;11 (Table 7). At age 17;11, Adam was given 64 items on this test (the final six items were not presented due to technical difficulties). Adam scored more than 2 SD below a reported young adult mean in both test administrations (Emmorey & Petrich, 2012), with 27 items (42.1%) and 31 items (44.2%) correct on the two administrations, respectively.
Adam's performance on the Fingerspelling Reproduction Test
| Age (years;months) | Adam% correct | Adam's score compared to adult means |
|---|---|---|
| 17;11 | 37% | <2 SD |
| 19;6 | 44% | <2 SD |
| Age (years;months) | Adam% correct | Adam's score compared to adult means |
|---|---|---|
| 17;11 | 37% | <2 SD |
| 19;6 | 44% | <2 SD |
Note: deaf adults (n = 36), (Mpercent correct = 82%; SD = 18%).
Adam's performance on the Fingerspelling Reproduction Test
| Age (years;months) | Adam% correct | Adam's score compared to adult means |
|---|---|---|
| 17;11 | 37% | <2 SD |
| 19;6 | 44% | <2 SD |
| Age (years;months) | Adam% correct | Adam's score compared to adult means |
|---|---|---|
| 17;11 | 37% | <2 SD |
| 19;6 | 44% | <2 SD |
Note: deaf adults (n = 36), (Mpercent correct = 82%; SD = 18%).
At 17;11, Adam's fingerspelling errors occurred mostly with real words longer than six letters and nonsense words longer than three letters. The majority of his error responses exhibited partial forms (e.g., missing letters) or incorrect ordering of letters, and for three items he simply responded “I don't know” (stenerous [nonsense word], acquaintance, and omniscient). In the following year, at 18;11, Adam attempted a response to all 70 test items presented and all three and four-letter words and non-words were spelled correctly, except for one four-letter item that is a nonsense word (jong). The two longest words that he spelled correctly were sixteen and mansion, but incorrect ordering of letters was still prevalent in his attempts at longer words. At 18;11, the following five-letter words were spelled incorrectly: scene, cough, and knead, the following six-letter words were spelled incorrectly: second, garage, saucer, toping, and accept, and once again the longest words spelled correctly were: sixteen and mansion. No words with more than seven letters were spelled correctly, and only two seven-letter words were spelled correctly. In both administrations, Adam made more errors with real words, but there was a greater percentage of longer real words than longer nonsense words on the test.
Other observed fingerspelling difficulties were made when Adam, age 19;6, was presented with 42 real words from the Fingerspelling Reproduction Test that were embedded within an ASL narrative. In this context, Adam provided a sign equivalent and definition for 14 (33%) of the fingerspelled words. These 14 words could be considered very common words (e.g., R-A-I-N, T-A-B-L-E, F-L-O-O-R) or lexicalized fingerspelling (e.g., #EARLY, #WAS, #WHEN). Of the remaining 28 (63.6%) items, Adam responded to 8 (18.1%) items with some description that indicated he may have guessed the meaning of the fingerspelled word, likely inferred from the contextual cues, but he could not provide a sign equivalent. Adam did not provide any guesses for 20 (48%) items, even though they were embedded within an ASL narrative.
Assessment of English Reading and Writing Skills
Throughout Adam's school years, he was given standardized psychoeducational assessments covering the following domains: Vocabulary, Reading Comprehension, Language, and Spelling (Table 8). During each evaluation between the ages of 11;10 and 15;10, he performed significantly below his hearing and deaf age peers on all domains. Adam completed standardized tests of English that were designed for the school districts in his home state when he was 16;5 (Table 9). He failed each of the English tests with a score significantly below the state passing cutoff.
Adam's Performance on General Standardized Tests of English
| Age (years;months) | Domain | Test | Score | GE | DE |
|---|---|---|---|---|---|
| 11;10 | Word Reading/Vocabulary | Stanford Achievement Test | 30% | 1.7 | −3.8 |
| Reading Comprehension | Stanford Achievement Test | 20% | Below measureable | No info | |
| Language | Stanford Achievement Test | Language = 43% | 1.8 | −3.7 | |
| Language Mechanics = 45% | |||||
| Expressions = 30% | |||||
| Spelling | Stanford Achievement Test | ABC order = 100% | 2.6 | −2.9 | |
| Spelling = 37% | |||||
| Sight Words = 40% | |||||
| Phonetic = 29% | |||||
| Structural = 50% | |||||
| 12;10 | Vocabulary | Trophies Placement and Diagnostic Assessment | Level 2–1 = 3/10 | Below second grade | −4.5+ |
| Level 2–2 = 5/10 | |||||
| Level 3–1 = 3/10 | |||||
| Total = 11/30 | |||||
| Comprehension | Trophies Placement and Diagnostic Assessment | Level 2–1 = 5/8 | Below second grade | −4.5+ | |
| Level 2–2 = 1/8 | |||||
| Level 3–1 = 3/8 | |||||
| Total = 9/24 | |||||
| 14;4 | Letter-Word Identification | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 50 | 2.1 | −5.9 (*−6.11) |
| Reading Fluency | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 66 | 2.1 | −5.9 (*−6.10) | |
| Passage Comprehension | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 54 | 1.9 | −6.1 (*−7.1) | |
| Broad Reading | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = Range of 53–57 | No info | No info | |
| Percentile Rank = <1% | |||||
| Overall Reading Ability Negligible | |||||
| Written Language | Oral and Written Language Scales | Standard Score = 66 | 2.6 | −5.4 | |
| 15;11 | Reading Vocabulary | Stanford Achievement Test | 33% | 1.5 | −8.0 |
| D/HH Percentile = 10 | |||||
| Reading Comprehension | Stanford Achievement Test | 48% | 1.9 | −7.6 | |
| D/HH Percentile = 25 | |||||
| Language | Stanford Achievement Test | 69% | 2.3 | −7.2 | |
| D/HH Percentile = 30 |
| Age (years;months) | Domain | Test | Score | GE | DE |
|---|---|---|---|---|---|
| 11;10 | Word Reading/Vocabulary | Stanford Achievement Test | 30% | 1.7 | −3.8 |
| Reading Comprehension | Stanford Achievement Test | 20% | Below measureable | No info | |
| Language | Stanford Achievement Test | Language = 43% | 1.8 | −3.7 | |
| Language Mechanics = 45% | |||||
| Expressions = 30% | |||||
| Spelling | Stanford Achievement Test | ABC order = 100% | 2.6 | −2.9 | |
| Spelling = 37% | |||||
| Sight Words = 40% | |||||
| Phonetic = 29% | |||||
| Structural = 50% | |||||
| 12;10 | Vocabulary | Trophies Placement and Diagnostic Assessment | Level 2–1 = 3/10 | Below second grade | −4.5+ |
| Level 2–2 = 5/10 | |||||
| Level 3–1 = 3/10 | |||||
| Total = 11/30 | |||||
| Comprehension | Trophies Placement and Diagnostic Assessment | Level 2–1 = 5/8 | Below second grade | −4.5+ | |
| Level 2–2 = 1/8 | |||||
| Level 3–1 = 3/8 | |||||
| Total = 9/24 | |||||
| 14;4 | Letter-Word Identification | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 50 | 2.1 | −5.9 (*−6.11) |
| Reading Fluency | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 66 | 2.1 | −5.9 (*−6.10) | |
| Passage Comprehension | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 54 | 1.9 | −6.1 (*−7.1) | |
| Broad Reading | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = Range of 53–57 | No info | No info | |
| Percentile Rank = <1% | |||||
| Overall Reading Ability Negligible | |||||
| Written Language | Oral and Written Language Scales | Standard Score = 66 | 2.6 | −5.4 | |
| 15;11 | Reading Vocabulary | Stanford Achievement Test | 33% | 1.5 | −8.0 |
| D/HH Percentile = 10 | |||||
| Reading Comprehension | Stanford Achievement Test | 48% | 1.9 | −7.6 | |
| D/HH Percentile = 25 | |||||
| Language | Stanford Achievement Test | 69% | 2.3 | −7.2 | |
| D/HH Percentile = 30 |
Note: GE = grade equivalent, DE = Difference from expected grade level (in years), (*x.x) = school records reported age equivalent different from expected age (in years.tenths-of-years), Stanford 10 = DHH norms (highlighted in bold font), all other tests = hearing norms.
Adam's Performance on General Standardized Tests of English
| Age (years;months) | Domain | Test | Score | GE | DE |
|---|---|---|---|---|---|
| 11;10 | Word Reading/Vocabulary | Stanford Achievement Test | 30% | 1.7 | −3.8 |
| Reading Comprehension | Stanford Achievement Test | 20% | Below measureable | No info | |
| Language | Stanford Achievement Test | Language = 43% | 1.8 | −3.7 | |
| Language Mechanics = 45% | |||||
| Expressions = 30% | |||||
| Spelling | Stanford Achievement Test | ABC order = 100% | 2.6 | −2.9 | |
| Spelling = 37% | |||||
| Sight Words = 40% | |||||
| Phonetic = 29% | |||||
| Structural = 50% | |||||
| 12;10 | Vocabulary | Trophies Placement and Diagnostic Assessment | Level 2–1 = 3/10 | Below second grade | −4.5+ |
| Level 2–2 = 5/10 | |||||
| Level 3–1 = 3/10 | |||||
| Total = 11/30 | |||||
| Comprehension | Trophies Placement and Diagnostic Assessment | Level 2–1 = 5/8 | Below second grade | −4.5+ | |
| Level 2–2 = 1/8 | |||||
| Level 3–1 = 3/8 | |||||
| Total = 9/24 | |||||
| 14;4 | Letter-Word Identification | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 50 | 2.1 | −5.9 (*−6.11) |
| Reading Fluency | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 66 | 2.1 | −5.9 (*−6.10) | |
| Passage Comprehension | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 54 | 1.9 | −6.1 (*−7.1) | |
| Broad Reading | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = Range of 53–57 | No info | No info | |
| Percentile Rank = <1% | |||||
| Overall Reading Ability Negligible | |||||
| Written Language | Oral and Written Language Scales | Standard Score = 66 | 2.6 | −5.4 | |
| 15;11 | Reading Vocabulary | Stanford Achievement Test | 33% | 1.5 | −8.0 |
| D/HH Percentile = 10 | |||||
| Reading Comprehension | Stanford Achievement Test | 48% | 1.9 | −7.6 | |
| D/HH Percentile = 25 | |||||
| Language | Stanford Achievement Test | 69% | 2.3 | −7.2 | |
| D/HH Percentile = 30 |
| Age (years;months) | Domain | Test | Score | GE | DE |
|---|---|---|---|---|---|
| 11;10 | Word Reading/Vocabulary | Stanford Achievement Test | 30% | 1.7 | −3.8 |
| Reading Comprehension | Stanford Achievement Test | 20% | Below measureable | No info | |
| Language | Stanford Achievement Test | Language = 43% | 1.8 | −3.7 | |
| Language Mechanics = 45% | |||||
| Expressions = 30% | |||||
| Spelling | Stanford Achievement Test | ABC order = 100% | 2.6 | −2.9 | |
| Spelling = 37% | |||||
| Sight Words = 40% | |||||
| Phonetic = 29% | |||||
| Structural = 50% | |||||
| 12;10 | Vocabulary | Trophies Placement and Diagnostic Assessment | Level 2–1 = 3/10 | Below second grade | −4.5+ |
| Level 2–2 = 5/10 | |||||
| Level 3–1 = 3/10 | |||||
| Total = 11/30 | |||||
| Comprehension | Trophies Placement and Diagnostic Assessment | Level 2–1 = 5/8 | Below second grade | −4.5+ | |
| Level 2–2 = 1/8 | |||||
| Level 3–1 = 3/8 | |||||
| Total = 9/24 | |||||
| 14;4 | Letter-Word Identification | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 50 | 2.1 | −5.9 (*−6.11) |
| Reading Fluency | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 66 | 2.1 | −5.9 (*−6.10) | |
| Passage Comprehension | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = 54 | 1.9 | −6.1 (*−7.1) | |
| Broad Reading | Woodcock–Johnson III Test of Achievement, Form A | Standard Score = Range of 53–57 | No info | No info | |
| Percentile Rank = <1% | |||||
| Overall Reading Ability Negligible | |||||
| Written Language | Oral and Written Language Scales | Standard Score = 66 | 2.6 | −5.4 | |
| 15;11 | Reading Vocabulary | Stanford Achievement Test | 33% | 1.5 | −8.0 |
| D/HH Percentile = 10 | |||||
| Reading Comprehension | Stanford Achievement Test | 48% | 1.9 | −7.6 | |
| D/HH Percentile = 25 | |||||
| Language | Stanford Achievement Test | 69% | 2.3 | −7.2 | |
| D/HH Percentile = 30 |
Note: GE = grade equivalent, DE = Difference from expected grade level (in years), (*x.x) = school records reported age equivalent different from expected age (in years.tenths-of-years), Stanford 10 = DHH norms (highlighted in bold font), all other tests = hearing norms.
Adam's Performance on a State-based Standardized Test of English (Hearing Norms)
| Age (years;months) | Subject | Score | Passing Score | State Average Score |
|---|---|---|---|---|
| 16;5 | Reading Vocabulary | 22 | 68 | 80 |
| 16;5 | Reading Comprehension | 22 | 63 | 77 |
| 16;5 | Literature Response and Analysis | 24 | 67 | 79 |
| 16;5 | Writing Process | 21 | 65 | 80 |
| 16;5 | Writing Applications | 16 | 58 | 67 |
| 16;5 | Language Conventions | 25 | 66 | 80 |
| Age (years;months) | Subject | Score | Passing Score | State Average Score |
|---|---|---|---|---|
| 16;5 | Reading Vocabulary | 22 | 68 | 80 |
| 16;5 | Reading Comprehension | 22 | 63 | 77 |
| 16;5 | Literature Response and Analysis | 24 | 67 | 79 |
| 16;5 | Writing Process | 21 | 65 | 80 |
| 16;5 | Writing Applications | 16 | 58 | 67 |
| 16;5 | Language Conventions | 25 | 66 | 80 |
Adam's Performance on a State-based Standardized Test of English (Hearing Norms)
| Age (years;months) | Subject | Score | Passing Score | State Average Score |
|---|---|---|---|---|
| 16;5 | Reading Vocabulary | 22 | 68 | 80 |
| 16;5 | Reading Comprehension | 22 | 63 | 77 |
| 16;5 | Literature Response and Analysis | 24 | 67 | 79 |
| 16;5 | Writing Process | 21 | 65 | 80 |
| 16;5 | Writing Applications | 16 | 58 | 67 |
| 16;5 | Language Conventions | 25 | 66 | 80 |
| Age (years;months) | Subject | Score | Passing Score | State Average Score |
|---|---|---|---|---|
| 16;5 | Reading Vocabulary | 22 | 68 | 80 |
| 16;5 | Reading Comprehension | 22 | 63 | 77 |
| 16;5 | Literature Response and Analysis | 24 | 67 | 79 |
| 16;5 | Writing Process | 21 | 65 | 80 |
| 16;5 | Writing Applications | 16 | 58 | 67 |
| 16;5 | Language Conventions | 25 | 66 | 80 |
A psychoeducational evaluation was administered to Adam at the age of 17;11 during the neuropsychological evaluation. On the Woodcock–Johnson Reading Fluency subtest, he performed at the level expected of a 8.4-year-old child (grade equivalent of 3.0). Adam responded “yes” to the following two questions: “A butterfly has ten wings” and “A shoe goes on your head.” He responded “no” for the sentence “A clock tells time.” On the Woodcock–Johnson Writing fluency subtest, he performed at the level expected of a 7.11-year-old child (grade equivalent of 2.3). When given three target words and asked to write sentences with those words, Adam provided various ungrammatical and unclear constructions. Examples are: “A dog food, then eat,” came from dog, food, and eats, “The little is foot,” was produced based on the, foot, and little, and “A cat with plays,” was generated from plays, cat, and with. He even had difficulty copying some of the words. For example, for the word “this,” he wrote “that.” Additionally, some spelling errors were found in his writing samples such as spelling “father” as “fathat.” These errors place his performance at the second grade level.
Discussion
Adam is a good candidate for an SLI diagnosis, considering the proposed adaptations to the diagnostic criteria based on the visual–gestural modality. Without a doubt, Adam meets the criterion for language impairment based on his ASL-SRT and fingerspelling test scores falling far greater than −1.25 SD below the performance of his peers despite have being raised in a rich ASL environment all his life. He also met nonlinguistic criteria as his nonverbal IQ was higher than 85; had no visual difficulties; had no neurological dysfunction; had no structural abnormalities of the face; arms, hands, or fingers; had no gross motor difficulties; and had no symptoms of impaired reciprocal social interaction. Symptoms of ADHD were not evident in the neuropsychological evaluation. However, he had notable memory and sequential processing difficulties. The SLI diagnostic criteria do not exclude children with memory and sequential processing difficulties from exhibiting an SLI. Hearing children with spoken language SLIs sometimes also have memory and sequential processing difficulties (e.g., Kushnir & Blake, 1996).
In some ways, Adam's profile differs somewhat from previously described cases of suggested SLI among BSL users (Herman et al., 2014; Marshall et al, 2006; Mason et al, 2010; Morgan et al., 2007). In those cases, the individuals struggled with complex morphological constructions in BSL similar to linguistic deficits associated with spoken language SLI. By contrast, we observed that Adam was successful in his production of a majority of ASL morpho-syntactic structures when engaged in natural conversation without lengthy turns or high syntactic complexity. However, Adam's performance on the ASL-SRT mirrors what was reported for SLI-diagnosed child signers of BSL (Marshall et al, 2014). This confirms the utility of sentence repetition, with increasing length and complexity, as one metric for determining language deficit in the sign modality. Of particular importance in Adam's case concerns the administration of ASL and fingerspelling measures that require sequential memory; when administered such tests, Adam's language impairment was obvious.2 This paradox is best explained by a further examination of Adam's performance on nonlinguistic cognitive tasks that require sequential processing. On several tests of short-term memory that involve remembering sequences of items (e.g., Digit Span Subtest) Adam scored poorly. Adam's scores were worse than expected of a deaf individual who was exposed to ASL since infancy.
Adam's case provides further evidence for a diversity of profiles of linguistic deficit in the signed modality. When compared with previous work on deaf children with language impairment, both from the UK (Marshall et al., 2006, 2013, 2015; Mason et al., 2010; Morgan et al., 2007) and from the US (e.g., Quinto-Pozos et al., 2011, 2013), the present case highlights the importance of considering nonlinguistic cognitive abilities (e.g., sequential memory) and their role in linguistic processing. In an earlier study of an ASL-signing deaf child (Quinto-Pozos et al., 2013), it was shown that deficits with visual–spatial processing (specifically, perspective taking) can have a notable effect on the acquisition of a sign language for a deaf child. In that case study, “Alice” showed signs of a visual–spatial deficit (in particular, perspective taking), which coincided with deficits in classifier production and processing and the production of role shifting. That study provided evidence for the strong ties between visual–spatial and linguistic development for the young signer. The heterogeneity of linguistic deficit in the signed modality is not unlike that for spoken language (Bishop, 2006).
Adam's performance on memory tasks reveals both strengths and weaknesses. He scored within the Average range on various assessments (e.g., the TVPS Visual Memory Test, the WMS Spatial Span Subtest, and the Mental Rotation Test), whereas he scored in the Low Average or Impaired range on others (e.g., three distinct tests of Immediate Recall). In those tests with Immediate and Delayed Recall, his performance improved (from Impaired to either Low Average or Average) in the Delayed Recall component. Standard administration procedures were followed for the tests that involved Immediate and Delayed recall, which mean that Adam was not shown the stimuli a second time. He was just asked to recall the items 20–30 minutes after the immediate recall. We are compelled to consider these results carefully among his performance on other standardized tests.
First, we discuss Adam's average performance. On the TVPS Visual Memory Test, the test taker is shown a design for 5 seconds and then shown several choices of designs and asked to choose the same as what was just seen. This approach does not test the sequencing of information, and Adam performed within the Average range. The WMS Spatial Span Subtest, a test of visual working memory involving a sequence of touches to images in distinct spaces, on which Adam performed within the Average range, does support the fact that Adam can remember sequences of information, especially when the sequentially provided bits of information are matched with distinct locations in space. It has been suggested that the WMS Spatial Span Subtest does not tap into the same processes as the Digit Span subscale (Wilde & Stauss, 2002), which is a well-known measure of short-term memory of sequential items. The WMS Spatial Span Subtest does also not require phonological encoding since the stimuli are nonlinguistic. Finally, the Mental Rotation Test is a visual working memory task that does not necessarily involve remembering a sequence of images. Rather, for this task, the test taker must be able to imagine a new orientation of a single image that was viewed. Adam performed in the Average range on this test too.
Next, we address Adam's poor performance. On the three tests that involve both Immediate and Delayed Recall, Adam performed comparably worse on the Immediate recall portion of the task. This suggests that Adam struggles to remember new items if tested immediately, especially if sequencing is involved (e.g., how a complex image could be organized in a sequence of steps, such as the Rey–Osterrieth Complex Figure test), but he is able to retain what he has viewed and recreate it after a delayed period of time.3 Consideration of all these results carefully shows that Adam does not struggle with all aspects of memory, but rather those that are related to immediately remembering a sequence of sequentially presented bits of information or information that needs to be organized and presented in sequences (e.g., the Rey–Osterrieth Complex Figure Test).
Adam's issues with sequential memory were also revealed in the ASL measures that involve sequencing skills (the ASL-SRT and the Fingerspelling Reproduction Test). The ASL-SRT requires that the test taker remember an entire sequence of signs within the sentence and immediately reproduce the signs and sequence verbatim. The Fingerspelling Reproduction Test is similar, although the focus is on English words and non-words as expressed manually via ASL handshapes and movements (as representations of English letters). Recall that on the ASL-PA, Adam's issues with memory and sequencing of signs were not observed. We argue this is because this language measure is conversationally based and involves no memory or sequencing task. We did note, however, that Adam's fingerspelling production throughout the ASL-PA sessions was noticeably infrequent and limited to short words or highly familiar or lexicalized forms, including proper nouns for entities that he is very familiar with.
As with most deaf children in the United States who sign, Adam was not exposed to only one language as a child: he was also learning English. Yet, Adam demonstrated clear difficulties with all measures of English literacy administered, scoring significantly behind his age-matched peers—both hearing and deaf/hard of hearing. Even as an adolescent, Adam did not seem to reach beyond a second or third grade reading level. Whereas, various studies have reported that deaf and hard of hearing (DHH) children often score below their hearing peers of tests of reading (e.g., see Enns & Lafond, 2007 for a brief review), Adam's performance on English measures is far below what would be expected of a native signing child (see studies cited above). We suggest that Adam's struggles with English are related to his weak sequencing and memory skills and the associated impact on his fingerspelling skills. Even when ASL context is provided to support fingerspelling comprehension, Adam does not derive the predictive benefit that is afforded to most bilingual learners of ASL and English (Humphries & MacDougall, 1999). Adam was not successful in committing many English words to long-term memory, which has drastically affected his literacy. Research with hearing children diagnosed with SLI suggests that such learners often have difficulty with the development of reading skills (e.g., Catts, Fey, Tomblin, & Zhang, 2002, among others). Whether Adam would have performed as poorly with reading if he were a hearing child acquiring English is a question that cannot be addressed by this study, but we suggest that Adam's struggles with reading have been influenced by his weaknesses with regard to memory and sequencing. It may be the case that Adam is a candidate for a secondary diagnosis of developmental dyslexia (e.g., see Enns & Lafond, 2007), but additional testing would need to be conducted to explore this possibility. It is not uncommon for literacy difficulties to co-occur with language impairment (Dockrell & Connelly, 2009).
One goal of this data presentation is to provide information about various aspects of a deaf bilingual child's abilities: English-through-reading, ASL, Fingerspelling (aspects of both English and ASL), and neuropsychological development. Table 10 provides a summary of the measures that comprise the data reported in this work.
Longitudinal Summary of Adam's Testing
| Domain | 11;10 | 12;10 | 14;4 | 15;10 | 16;5 | 17;11 | 18;11 | 19;6 |
|---|---|---|---|---|---|---|---|---|
| English | Stanford Achievement | Trophies Placement | WJ, OWLS | Stanford Achievement | State Tests | |||
| ASL | ASL-PA | ASL-SRT | ASL-SRT | ASL-SRT | ||||
| Fingerspelling | FS | FS, FS adapted | ||||||
| Neuropsychological | Battery |
| Domain | 11;10 | 12;10 | 14;4 | 15;10 | 16;5 | 17;11 | 18;11 | 19;6 |
|---|---|---|---|---|---|---|---|---|
| English | Stanford Achievement | Trophies Placement | WJ, OWLS | Stanford Achievement | State Tests | |||
| ASL | ASL-PA | ASL-SRT | ASL-SRT | ASL-SRT | ||||
| Fingerspelling | FS | FS, FS adapted | ||||||
| Neuropsychological | Battery |
Note: ASL-PA = ASL Proficiency Assessment; ASL-SRT = ASL Sentence Reproduction Test; FS = Fingerspelling Reproduction Test; OWLS = Oral and Written Language Scales; WJ = Woodcock–Johnson Test of Achievement.
Longitudinal Summary of Adam's Testing
| Domain | 11;10 | 12;10 | 14;4 | 15;10 | 16;5 | 17;11 | 18;11 | 19;6 |
|---|---|---|---|---|---|---|---|---|
| English | Stanford Achievement | Trophies Placement | WJ, OWLS | Stanford Achievement | State Tests | |||
| ASL | ASL-PA | ASL-SRT | ASL-SRT | ASL-SRT | ||||
| Fingerspelling | FS | FS, FS adapted | ||||||
| Neuropsychological | Battery |
| Domain | 11;10 | 12;10 | 14;4 | 15;10 | 16;5 | 17;11 | 18;11 | 19;6 |
|---|---|---|---|---|---|---|---|---|
| English | Stanford Achievement | Trophies Placement | WJ, OWLS | Stanford Achievement | State Tests | |||
| ASL | ASL-PA | ASL-SRT | ASL-SRT | ASL-SRT | ||||
| Fingerspelling | FS | FS, FS adapted | ||||||
| Neuropsychological | Battery |
Note: ASL-PA = ASL Proficiency Assessment; ASL-SRT = ASL Sentence Reproduction Test; FS = Fingerspelling Reproduction Test; OWLS = Oral and Written Language Scales; WJ = Woodcock–Johnson Test of Achievement.
Early information, before we began to work with Adam, comes primarily in the form of the results of standardized tests of English. Over a period of approximately 5 years (11;10–16;5), Adam's English scores were between three and eight grade equivalents lower than expected for his chronological age. Data from his mid-to-late teens (15;10–19;6) focus mostly on ASL, Fingerspelling, and neuropsychological measures. On the ASL and fingerspelling measures, Adam improved slightly over a roughly 2-year period (17;11–19;6), but they remained far below what would be expected for a native signing deaf child (and below comparable data from deaf peers reported elsewhere). Repeated administrations of these normed instruments over multiple years were intended to assess improvement over time. Some assessments (e.g., ASL-PA sessions) were administered once, simply because they were not as designed to challenge a child's memory and sequencing—unlike the ASL-SRT and Fingerspelling Reproduction Test. The conversational nature of the ASL-PA data collection sessions was not ideal for assessing memory abilities, as was shown by Adam's average performance using that instrument. During the entire period, modest gains in ASL might be attributed to continued work with tutors, language specialists (e.g., Speech and Language Therapists), and teachers. Age may have played some role, as well, and it is also the case that memory from previous administrations (e.g., remembering a specific word that appeared on the Fingerspelling Reproduction Test) could have boosted performance. However, the involvement of his mother in his development should not be overlooked in the improvement that was achieved by Adam. It is likely that support from home and school helped him, but Adam's deficits were difficult to overcome.
One possible account for Adam's profile is that the highly simultaneous structure of ASL and his intact memory and processing capacities for visual–spatial information have allowed for the acquisition of many features of the language, even though he may have undergone protracted development in one or more areas. However, his weakness with short-term memory for sequential information appears to have impacted his ASL processing when he is expected to hold lengthy sentences in short-term memory (the effect of this may be most noticeable in academic settings when a student is asked to memorize and recall exemplars of teacher-presented information). He had difficulty on structures that are more characteristically sequential and segmental, namely fingerspelling. He may be less able to process lengthy fingerspelled forms because of his sequential processing deficit and also may be less able to engage in the process of holding an ASL sentence in short-term memory, breaking it down sequentially, and finding English equivalents. For these reasons, it is possible his English proficiency has been negatively affected.
Adam's language and clinical profile raises questions about how such cases might be treated by educators and language specialists at residential and mainstream schools. We speculate that a diagnostic category that has been used primarily for research purposes (e.g., SLI) might not be regularly employed in school settings. Rather, the focus by diagnosticians may be on a broader classification of language impairment (e.g., Language Disorder or Unspecified Communication Disorder, as specified in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; American Psychological Association, 2013) that would allow the school to create a plan for intervention.4 It is not uncommon for educators and language professionals familiar with DHH children to encounter a broad range of signed language abilities among their students, due in great part to late exposure to a sign language for the vast majority of such children (Mitchell & Karchmer, 2004). Additionally, there is also the question about comorbidity with additional diagnoses such as autism spectrum disorder (e.g., see Szymankski, Brice, Lam, & Hotto, 2012; Shield & Meier, 2014) and ADHD (Guardino, 2008; Knoors & Vervloed, 2003). It may be the case that the complexity of accurate diagnosis is overwhelming for some educators and clinicians. We, nonetheless, urge educators and clinicians to carefully consider a child's performance using multiple measures—both linguistic and nonlinguistic—to determine if a child's deficit is much broader than linguistic in nature (i.e., a non-SLI) versus one that primarily affects linguistic abilities (i.e., SLI), such as the present case.
Conclusion
Adam is a native signer who grew up in a signing household and attended an ASL/English bilingual school for the deaf for all of his schooling. He has average intelligence, intact visual perceptual and motor skills, unremarkable social skills, and no significant emotional difficulties beyond frustration with language. His ASL skills might not appear atypical to a person just meeting him, engaged in casual ASL conversation, unless fingerspelling is used. This detailed case study reveals that he has a history of marked sign language difficulties that began early in his life, and they appear to be related to his challenges with sequencing and memory. Detailed information about Adam through school personnel and from his parent, and the results of linguistic and nonlinguistic assessments, suggests that a deaf signer can be a candidate for an SLI diagnosis.
This study proposes diagnostic criteria for children with noticeable signed language acquisition problems to be considered as candidates for an SLI diagnosis. Rather than rule out a child without intact hearing for a possible diagnosis of SLI, we suggest that researchers and clinicians consider the suggested adaptation of the SLI diagnostic criteria. There is a need for the further development of instruments that can appropriately assess these skills in deaf signers to improve our ability to more accurately diagnose the underlying cause of their language difficulties and develop more appropriate strategies for therapeutic intervention. Work on SLI in different language modalities also contributes to our scientific understanding of the role of modality and nonlinguistic cognition in language impairment.
Funding
This research was supported by the National Science Foundation Science of Learning Center Program, under cooperative agreement number SBE-0541953.
Conflicts of Interest
No conflicts of interest were reported.
Notes
This estimate is lower than other studies of language disorder in deaf signing children (e.g., Mason et al., 2010), where researchers have suggested that the incidence of SLI among deaf children who sign BSL is similar to what has been reported for hearing children (e.g., Leonard, 1998). The lower estimate in our study may be due to differences between residential and mainstream schools and/or imprecise estimates of the language professionals based on multiple years of experience.
Adam's fingerspelling performance is reminiscent of the error reported by one of the SLI children in the Marshall et al. (2013) study. As noted earlier, a child struggled with fingerspelling simple words (e.g., G-G-E-E instead of E-G-G).
Data from immediate versus delayed recall might suggest that Adam is experiencing an issue of memory consolidation, which relates to the memory trace that is created at the initial acquisition of a memory. We thank our colleague, Matt Hall, for this insightful comment. Unfortunately, we do not have other data to address this possibility.
See Reilly et al. (2014) for an argument in favor of non-inclusion of the term “SLI” in the DSM-5. The authors point out that the label has been widely used by researchers, but it is less useful for clinicians and other service providers.
Acknowledgments
Any opinions, findings, and conclusions or recommendations expressed are those of the authors and do not necessarily reflect the views of the National Science Foundation. The authors would like to thank Carrie Lou Garberoglio and Lynn Hou for their work on this project, and Matt Hall for comments on a previous draft of this manuscript.
References
Appendix A
Fingerspelled words from The Fingerspelling Reproduction Test embedded within an ASL narrative.
ASL: A School Day
(English translation of ASL narrative; fingerspelled words are indicated in bold font)
Today I woke up, looked outside the window and saw rain, which meant that the soccer game would be canceled. I felt today would not be a good day. My mom tried to coax me out of bed by telling me that the bacon had been cooked and the bread had been baked. She got up early in the morning to knead the bread. I love homemade bread! I sat at the table and ate the bread but it was hard like concrete!
When I got to school, my English teacher told us that we had a surprise quiz! All of us were unanimous in our decision to not accept the surprise. I took the test, but couldn't remember the difference between an apostrophe and a comma! I also had to count how many syllable in the word vacillate and in the word acquaintance. I didn't know either! Another girl in my class knew all the answers- she must be omniscient! She always gets everything right and I was sick of her arrogance.
When English class was finished, we went to theater class and practiced our play. I was playing Cinderella for the play, so we decorated the stage like a fancy mansion. We even made a big carriage with sixteen horses. When it was my turn to do my scene, I walked in with my sparkly crystal shoes but the floor was slippery and I fell. I was embarrassed and wished for my disappearance.
I went to the cafeteria for lunch, and we had a green soup with different stuff in it that looked really bizarre. It was served with bread that was plain, no butter or anything. Yesterday the cafeteria lunch tasted awful, and today was the second straight day that I did not eat lunch.
I think that it's important that today is Friday since that's when we get rewards in art class and can watch a movie. The teacher tends to show my favorite kinds of movies, like adventure and fantasy films. I went in the classroom but I started to cough really loud. The teacher sent me to the nurse and the nurse told me that I had a throat inflammation and I had to go home and miss the movie.
When I got home, I got out of the car and left my backpack in the garage. I went in the house and my mom made me tea because my throat hurt. She put the teacup on a little saucer with a napkin under it. My mom was in a congenial mood and wanted to talk, but I did not feel like talking. Today was not a good day!

{kind=link}