




The aim of this study was to pilot a method of a small-scale survey for the assessment of Keshan disease (KD) elimination at township level.
The prevalence of chronic KD was obtained by case-searching the whole population. The endemic village with the highest prevalence of chronic KD was selected as the key village for the survey of latent KD prevalence rate among permanent residents. The selenium levels in the head hair of individuals in the key village was measured. The professionals of the department of endemic disease control, the township and village doctors were surveyed by pre-designed questionnaire survey for KD interventions.
We conducted this study in 2013. Yuanbao township had a population of 16 487 people and 14 862 permanent residents. There were no acute or subacute KD cases in the previous 5 years. The prevalence rate of chronic KD and natural chronic KD were 6.7/10 000 and 3.4/10 000 respectively. The prevalence rate of latent KD was 250.6/10 000, higher than the elimination criterion. The head hair selenium levels were 0.23±0.18 mg/kg.
The small-scale survey methodology for assessing KD elimination at township level was feasible. KD among the people living in Yuanbao township has not been eliminated.
Introduction
Keshan disease (KD) is an endemic cardiomyopathy.1 Although, its etiology is not fully known most researchers believe that selenium deficiency is a cause of KD, but not the only one.2–4 According to the type of attack, clinical features and heart function, KD is clinically divided into four categories: acute, subacute, chronic and latent KD disease.5 To date, KD has appeared in 2953 townships in 327 counties in 16 provinces.6 Because KD occurs only in specific selenium deficient rural areas in China, it is classified as an endemic disease in China, and these specific rural areas are delimitated as endemic areas of KD. There are 9289 rural townships in the 16 provinces, so the KD endemic townships account 31.8% (2953/9289). The smallest administrative unit in the endemic areas of KD is the township.
The peak incidence and prevalence were in the early 1960s, and acute KD had a fatality rate of 80–90%. Since the late 1970s, the KD incidence and prevalence rate has sharply declined.7 The results of the national KD surveillance also showed that no acute KD cases since 1990 and only six cases of subacute KD were found in Sichuan province in 2006, and the majority of the current KD cases have been chronic KD since 1990.8–10 As the prevalence rate of KD is now at a low level, the goal of KD prevention and control in the National Endemic Disease Prevention and Control Plan (2011–2015) in China is ‘basically eliminating Keshan disease, in 90% or more counties of the Keshan disease endemic areas to reach the criteria of Keshan disease elimination’.11 The KD elimination criteria involves two aspects: one is organization and management including the annual plan, institution, funds, instruments and equipment, the professional team, work summaries and project files of the KD intervention. The other is the technical indicators including that there are no acute or subacute KD patients in the last 5 years at the township level and the prevalence rate of chronic KD and latent KD are lower than 5 per 10 000 people and 90 per 10 000 people at township level, respectively.
This goal for the National Endemic Disease Prevention and Control Plan (2011–2015) in China raised a very challenging question: how do we assess KD elimination at the township level? Normally, the outcome of a disease surveillance is the way to assess the elimination of the disease. However, the role played by surveillance in the assessment of elimination is less direct. KD is not a notifiable disease, and its surveillance is generally active sentinel surveillance in methodology, which means that we are unable to answer the question with data and results of KD surveillance completed previously. It is necessary to collect the data of the whole population to be assessed. It is impossible, infeasible and unnecessary to perform a census of KD to get a population-based prevalence. The methodology for assessment of KD elimination is urgently needed. The approach clearly requires innovation in the multidisciplinary areas of disease surveillance of epidemiology, and assessment for KD elimination. In other words, we need to translate the needs of KD prevention and control to develop the methodology to feasibly assess KD elimination into the development of disease surveillance of epidemiology. The aim of this study is to pilot-test a method we developed for feasibly assessing KD elimination at the township level by a small-scale survey.
Methods
Study scope and design
The study was conducted in 2013 in Yuanbao township, Shangzhi County, Harbin City, Heilongjiang Province, China. The inclusion criteria was the length of residence: residents who had lived in the endemic areas for 6 months or more in the past 12 months were the subjects of this research.
The design of this study was comprehensive. It was composed of case-searching the whole population for acute, subacute and chronic KD cases; the key village survey for the latent KD; survey of the KD endemic scope and the population at risk; the level of selenium in the head hair of the male adults and boys living in the key village; and the information on KD interventions. The number of the chronic KD patients was obtained by case-searching in the whole population. The village with the highest prevalence of chronic KD was selected as the key village to represent the potentially highest prevalence rate of latent KD.
The KD interventions
The information on KD intervention in Shangzhi county was collected from the professionals of the Shangzhi County Centre for Disease Control and Prevention by questionnaire survey, including the annual plan, institution, funds, instrument, professional team, work summaries and project files of the KD intervention.
The endemic scope and the population
The information on endemic scope was collected from the Yuanbao township doctors. The population data were from the village doctors, who completed the pre-designed questionnaires including the data of name, sex, age, address, and permanent residency of the residents.
The chronic KD patients
The chronic KD patients present chronic heart failure and dilated chambers of the hearts; the heart walls become thinner than normal. Natural chronic KD is a type of chronic KD which has no history of acute KD, subacute KD and latent KD, but when patients see doctors they have already had typical clinical manifestation of chronic heart failure.
Searching the chronic KD cases was conducted by obtaining reports and searching the records of the cases of the county and township hospitals for the whole population. The information on chronic KD cases was obtained through three steps. First, all village doctors of the Yuanbao township reported the cases with cardiomyopathy by completing the Suspected Cases of KD form. Second, the suspected cases of KD were identified by the investigation team members by telephone interview of the suspected case for the medical history, clinical features, and epidemiological information with pre-designed questionnaires. Finally, the KD cases were confirmed at the township hospital by the medical team members of this study based on the results of medical examination, electrocardiograms (ECG), echocardiography and chest X-ray against the Criteria for Diagnosis of Keshan Disease (WS/T-2011).5
The key village survey
The prevalence of latent KD was obtained through the key village survey. The onset of latent KD is disguised, and the patients have reasonably good heart function (NYHA class I). Ventricular extrasystole and right bundle branch block or ST-T change are common. Cardiomegaly is not observed.
The endemic village with potentially the highest prevalence rate of chronic KD was selected as the key village according to the results of chronic KD survey and the clue of the epidemiological distribution of the KD patients which was provided by the chief physicians of departments of internal medicine, emergency, and pediatrics of the People's Hospital of Shangzhi County and the Yuanbao township hospital. The subjects of the key village survey were the permanent residents living in the village. All subjects underwent medical examination, ECG, echocardiography and a survey with predesigned questionnaires. After that the subjects with an abnormal ECG had chest X-ray examination. The cases of latent KD were diagnosed by the medical team of this study against the Criteria for Diagnosis of Keshan Disease (WS/T-2011).5
The head hair selenium
The selenium deficiency is a cause result of having KD. The selenium level of the head hairs of the residents living in the endemic areas of KD not only reflects the risk of having KD but also the effectiveness of prevention and control measures. In the key survey village, 10 adult males and 10 boys aged 10 year or younger were selected by convenience sampling and 2 g of hairs within 2 cm distance to the hair root on the occiput of the head were collected. The hair selenium content was measured with the hydride generation method of atomic fluorescence spectrometry.
Assessment of KD elimination
Firstly, the KD intervention was evaluated. Secondly, we checked for acute and subacute KD cases in the last 5 years. Thirdly, the prevalence rate of chronic KD of the whole population of the Yuanbao township and the prevalence rate of latent KD of the key village were compared to the elimination criteria of KD. Finally, assessment conclusion was drawn against the indictors of the KD elimination criteria.
Diagnostic criteria and investigation team
KD cases were confirmed by the medical team of this study according to the Criteria for Diagnosis of Keshan Disease (WS/T-2011).5
The team consisted of epidemiologists, cardiologists, ECG physicians, echocardiographic physician and X-ray technician, professional staff of the department of endemic disease prevention and control of the county CDC, the township and village doctors.
Statistical analysis
The data were analyzed by SPSS 17.0 for Windows (SPSS Inc, Chicago, IL, USA). The age and the head hair selenium level were statistically described by mean±standard deviation. The t-test was used for the difference significance of the head hair selenium levels between the samples of this study and the reference values.
Ethical approval
This study was carried out after getting ethical approval from the Ethical Review Board of Harbin Medical University. The interviewer fully explained the purpose of the study to each participant and obtained full verbal informed consent from each study participant before the interview and measurements. If minors or children enrolled in our study, informed consent was obtained from their guardians on their behalf.
Results
The KD interventions
The Shangzhi county government had a plan for KD prevention and control. The Shangzhi County CDC had undertaken the provincial project of KD prevention and control in the past 10 years, and the project documents are complete. The Shangzhi County CDC has an independent department and professional team for endemic disease prevention and control.
The endemic scope and the population
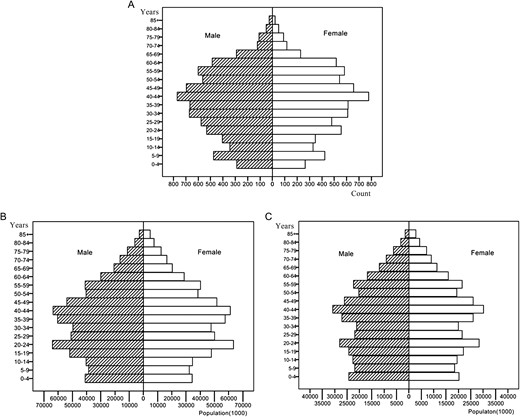
The population pyramids of (A) the Yuanbao township, (B) China national, and (C) China rural. The population data of China national and China rural on the 2010 population census of the people republic of China is cited in B and C.12
Prevalence rates of chronic KD
There were no acute or subacute KD cases in Yuanbao township in the last 5 years. In searching for cases of chronic KD, 31 suspected cases were found, but only 10 were confirmed. The prevalence rate of chronic KD was 6.7/10 000. Of the 10 chronic KD cases, five were natural chronic KD cases, and the prevalence rate was 3.4/10 000. The details are shown in Table 1.
The prevalence rate of Keshan Disease (KD) by type of KD by village and sex in Yuanbao township in 2013
| KD type and village | Subjects surveyed | Number of KD | Prevalence rate (1/10 000) | ||||||
| Male | Female | All | Male | Female | All | Male | Female | All | |
| Chronic KD | |||||||||
| Yuanbao | 1030 | 969 | 1999 | 1 | 1 | 2 | 9.7 | 10.3 | 10 |
| Xiangqianjin | 666 | 609 | 1275 | 1 | 2 | 3 | 15 | 32.8 | 23.5 |
| Yangshu | 830 | 755 | 1585 | 1 | 1 | 2 | 12 | 13.2 | 12.6 |
| Xinfa | 603 | 587 | 1190 | 0 | 0 | 0 | 0 | 0 | 0 |
| Xinnong | 364 | 369 | 733 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gangtie | 729 | 765 | 1494 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yangjiadian | 816 | 745 | 1561 | 1 | 1 | 2 | 12.3 | 13.4 | 12.8 |
| Dongfeng | 263 | 266 | 529 | 1 | 0 | 1 | 38 | 0 | 18.9 |
| Minren | 485 | 425 | 910 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yumin | 799 | 757 | 1556 | 0 | 0 | 0 | 0 | 0 | 0 |
| Anle | 609 | 530 | 1139 | 0 | 0 | 0 | 0 | 0 | 0 |
| Zhongxin | 468 | 423 | 891 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 7662 | 7200 | 14 862 | 5 | 5 | 10 | 6.5 | 6.9 | 6.7 |
| Natural chronic KD | |||||||||
| Yuanbao | 1030 | 969 | 1999 | 1 | 1 | 2 | 9.7 | 10.3 | 10.0 |
| Xiangqianjin | 666 | 609 | 1275 | 0 | 1 | 1 | 0 | 16.4 | 7.8 |
| Yangshu | 830 | 755 | 1585 | 1 | 0 | 1 | 12.0 | 0 | 6.3 |
| Xinfa | 603 | 587 | 1190 | 0 | 0 | 0 | 0 | 0 | 0 |
| Xinnong | 364 | 369 | 733 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gangtie | 729 | 765 | 1494 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yangjiadian | 816 | 745 | 1561 | 1 | 0 | 1 | 12.3 | 0 | 6.4 |
| Dongfeng | 263 | 266 | 529 | 0 | 0 | 0 | 0 | 0 | 0 |
| Minren | 485 | 425 | 910 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yumin | 799 | 757 | 1556 | 0 | 0 | 0 | 0 | 0 | 0 |
| Anle | 609 | 530 | 1139 | 0 | 0 | 0 | 0 | 0 | 0 |
| Zhongxin | 468 | 423 | 891 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 7662 | 7200 | 14 862 | 3 | 2 | 5 | 3.9 | 2.8 | 3.4 |
| Latent KD | |||||||||
| Key village | 150 | 249 | 399 | 4 | 6 | 10 | 266.7 | 241.0 | 250.6 |
| KD type and village | Subjects surveyed | Number of KD | Prevalence rate (1/10 000) | ||||||
| Male | Female | All | Male | Female | All | Male | Female | All | |
| Chronic KD | |||||||||
| Yuanbao | 1030 | 969 | 1999 | 1 | 1 | 2 | 9.7 | 10.3 | 10 |
| Xiangqianjin | 666 | 609 | 1275 | 1 | 2 | 3 | 15 | 32.8 | 23.5 |
| Yangshu | 830 | 755 | 1585 | 1 | 1 | 2 | 12 | 13.2 | 12.6 |
| Xinfa | 603 | 587 | 1190 | 0 | 0 | 0 | 0 | 0 | 0 |
| Xinnong | 364 | 369 | 733 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gangtie | 729 | 765 | 1494 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yangjiadian | 816 | 745 | 1561 | 1 | 1 | 2 | 12.3 | 13.4 | 12.8 |
| Dongfeng | 263 | 266 | 529 | 1 | 0 | 1 | 38 | 0 | 18.9 |
| Minren | 485 | 425 | 910 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yumin | 799 | 757 | 1556 | 0 | 0 | 0 | 0 | 0 | 0 |
| Anle | 609 | 530 | 1139 | 0 | 0 | 0 | 0 | 0 | 0 |
| Zhongxin | 468 | 423 | 891 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 7662 | 7200 | 14 862 | 5 | 5 | 10 | 6.5 | 6.9 | 6.7 |
| Natural chronic KD | |||||||||
| Yuanbao | 1030 | 969 | 1999 | 1 | 1 | 2 | 9.7 | 10.3 | 10.0 |
| Xiangqianjin | 666 | 609 | 1275 | 0 | 1 | 1 | 0 | 16.4 | 7.8 |
| Yangshu | 830 | 755 | 1585 | 1 | 0 | 1 | 12.0 | 0 | 6.3 |
| Xinfa | 603 | 587 | 1190 | 0 | 0 | 0 | 0 | 0 | 0 |
| Xinnong | 364 | 369 | 733 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gangtie | 729 | 765 | 1494 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yangjiadian | 816 | 745 | 1561 | 1 | 0 | 1 | 12.3 | 0 | 6.4 |
| Dongfeng | 263 | 266 | 529 | 0 | 0 | 0 | 0 | 0 | 0 |
| Minren | 485 | 425 | 910 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yumin | 799 | 757 | 1556 | 0 | 0 | 0 | 0 | 0 | 0 |
| Anle | 609 | 530 | 1139 | 0 | 0 | 0 | 0 | 0 | 0 |
| Zhongxin | 468 | 423 | 891 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 7662 | 7200 | 14 862 | 3 | 2 | 5 | 3.9 | 2.8 | 3.4 |
| Latent KD | |||||||||
| Key village | 150 | 249 | 399 | 4 | 6 | 10 | 266.7 | 241.0 | 250.6 |
The prevalence rate of Keshan Disease (KD) by type of KD by village and sex in Yuanbao township in 2013
| KD type and village | Subjects surveyed | Number of KD | Prevalence rate (1/10 000) | ||||||
| Male | Female | All | Male | Female | All | Male | Female | All | |
| Chronic KD | |||||||||
| Yuanbao | 1030 | 969 | 1999 | 1 | 1 | 2 | 9.7 | 10.3 | 10 |
| Xiangqianjin | 666 | 609 | 1275 | 1 | 2 | 3 | 15 | 32.8 | 23.5 |
| Yangshu | 830 | 755 | 1585 | 1 | 1 | 2 | 12 | 13.2 | 12.6 |
| Xinfa | 603 | 587 | 1190 | 0 | 0 | 0 | 0 | 0 | 0 |
| Xinnong | 364 | 369 | 733 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gangtie | 729 | 765 | 1494 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yangjiadian | 816 | 745 | 1561 | 1 | 1 | 2 | 12.3 | 13.4 | 12.8 |
| Dongfeng | 263 | 266 | 529 | 1 | 0 | 1 | 38 | 0 | 18.9 |
| Minren | 485 | 425 | 910 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yumin | 799 | 757 | 1556 | 0 | 0 | 0 | 0 | 0 | 0 |
| Anle | 609 | 530 | 1139 | 0 | 0 | 0 | 0 | 0 | 0 |
| Zhongxin | 468 | 423 | 891 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 7662 | 7200 | 14 862 | 5 | 5 | 10 | 6.5 | 6.9 | 6.7 |
| Natural chronic KD | |||||||||
| Yuanbao | 1030 | 969 | 1999 | 1 | 1 | 2 | 9.7 | 10.3 | 10.0 |
| Xiangqianjin | 666 | 609 | 1275 | 0 | 1 | 1 | 0 | 16.4 | 7.8 |
| Yangshu | 830 | 755 | 1585 | 1 | 0 | 1 | 12.0 | 0 | 6.3 |
| Xinfa | 603 | 587 | 1190 | 0 | 0 | 0 | 0 | 0 | 0 |
| Xinnong | 364 | 369 | 733 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gangtie | 729 | 765 | 1494 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yangjiadian | 816 | 745 | 1561 | 1 | 0 | 1 | 12.3 | 0 | 6.4 |
| Dongfeng | 263 | 266 | 529 | 0 | 0 | 0 | 0 | 0 | 0 |
| Minren | 485 | 425 | 910 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yumin | 799 | 757 | 1556 | 0 | 0 | 0 | 0 | 0 | 0 |
| Anle | 609 | 530 | 1139 | 0 | 0 | 0 | 0 | 0 | 0 |
| Zhongxin | 468 | 423 | 891 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 7662 | 7200 | 14 862 | 3 | 2 | 5 | 3.9 | 2.8 | 3.4 |
| Latent KD | |||||||||
| Key village | 150 | 249 | 399 | 4 | 6 | 10 | 266.7 | 241.0 | 250.6 |
| KD type and village | Subjects surveyed | Number of KD | Prevalence rate (1/10 000) | ||||||
| Male | Female | All | Male | Female | All | Male | Female | All | |
| Chronic KD | |||||||||
| Yuanbao | 1030 | 969 | 1999 | 1 | 1 | 2 | 9.7 | 10.3 | 10 |
| Xiangqianjin | 666 | 609 | 1275 | 1 | 2 | 3 | 15 | 32.8 | 23.5 |
| Yangshu | 830 | 755 | 1585 | 1 | 1 | 2 | 12 | 13.2 | 12.6 |
| Xinfa | 603 | 587 | 1190 | 0 | 0 | 0 | 0 | 0 | 0 |
| Xinnong | 364 | 369 | 733 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gangtie | 729 | 765 | 1494 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yangjiadian | 816 | 745 | 1561 | 1 | 1 | 2 | 12.3 | 13.4 | 12.8 |
| Dongfeng | 263 | 266 | 529 | 1 | 0 | 1 | 38 | 0 | 18.9 |
| Minren | 485 | 425 | 910 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yumin | 799 | 757 | 1556 | 0 | 0 | 0 | 0 | 0 | 0 |
| Anle | 609 | 530 | 1139 | 0 | 0 | 0 | 0 | 0 | 0 |
| Zhongxin | 468 | 423 | 891 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 7662 | 7200 | 14 862 | 5 | 5 | 10 | 6.5 | 6.9 | 6.7 |
| Natural chronic KD | |||||||||
| Yuanbao | 1030 | 969 | 1999 | 1 | 1 | 2 | 9.7 | 10.3 | 10.0 |
| Xiangqianjin | 666 | 609 | 1275 | 0 | 1 | 1 | 0 | 16.4 | 7.8 |
| Yangshu | 830 | 755 | 1585 | 1 | 0 | 1 | 12.0 | 0 | 6.3 |
| Xinfa | 603 | 587 | 1190 | 0 | 0 | 0 | 0 | 0 | 0 |
| Xinnong | 364 | 369 | 733 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gangtie | 729 | 765 | 1494 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yangjiadian | 816 | 745 | 1561 | 1 | 0 | 1 | 12.3 | 0 | 6.4 |
| Dongfeng | 263 | 266 | 529 | 0 | 0 | 0 | 0 | 0 | 0 |
| Minren | 485 | 425 | 910 | 0 | 0 | 0 | 0 | 0 | 0 |
| Yumin | 799 | 757 | 1556 | 0 | 0 | 0 | 0 | 0 | 0 |
| Anle | 609 | 530 | 1139 | 0 | 0 | 0 | 0 | 0 | 0 |
| Zhongxin | 468 | 423 | 891 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 7662 | 7200 | 14 862 | 3 | 2 | 5 | 3.9 | 2.8 | 3.4 |
| Latent KD | |||||||||
| Key village | 150 | 249 | 399 | 4 | 6 | 10 | 266.7 | 241.0 | 250.6 |
The results of the national KD surveillance in 2012 (a separate study, unpublished) showed that there were five chronic KD cases in Yuanbao village, three in Xiangqianjin village and two in Yangjiadian. The highest prevalence rate was in Xiangqianjin. In the chronic KD survey there were 10 cases, and the highest prevalence rate was also in Xiangqianjin in the present study in 2013. Therefore Xiangqianjin was selected as the key village. We surveyed 399 subjects in the key KD survey village, including 150 males and 249 females; their average age was 49.41±16.23 years. We found 10 cases of latent KD, and the prevalence was 250.6/10 000, including six females (241.0/10 000) and four males (266.7/10 000). The details are shown in Table 1.
The head hair selenium level
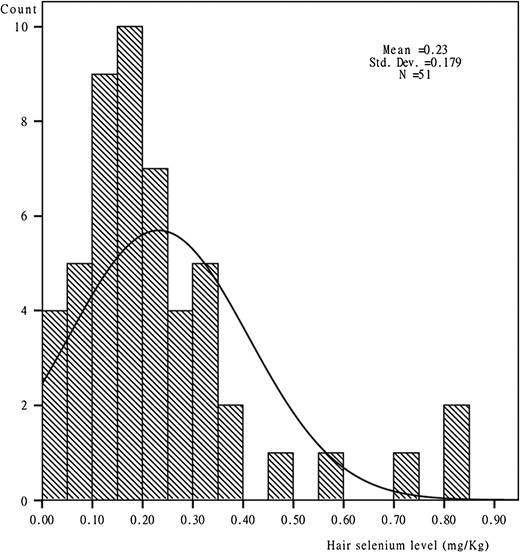
Head hair selenium levels in the key village in Yuanbao township in 2013.
The Shangzhi County CDC was well-organized and well-functioned for KD intervention. There was no acute and subacute KD and the prevalence rate of natural chronic KD was 3.4/10 000 in Yuanbao, which was lower than the 5/10 000 of the KD elimination criteria. The prevalence rate of latent KD was 250.6/10 000, which is higher than 90/10 000. Therefore, KD prevalence status among the residents living in Yuanbao township is close to, but has not reached, the criteria of KD elimination.
Discussion
Elimination was defined as ‘zero disease in a defined geographic area as a result of deliberate efforts’.15 People have concentrated on eliminating many diseases, including polio, measles and malaria, which are all notifiable diseases and their data are obtained by passive surveillance.16–18 However, KD is not a notifiable disease; the data can be obtained yearly by active surveillance. The national surveillance of KD played an important role in guiding KD prevention and control, but not all the outcomes of national KD surveillance can be used for assessment of KD elimination. In other words, assessment of KD elimination cannot be replaced by KD surveillance. The main reason for this is that, in concept, surveillance of a disease does not necessarily make the diagnosis of the status of the disease incident, prevalent or controlled in a defined population, and assessment of disease elimination must make this kind of diagnosis against the relevant criteria. In China, national surveillance of KD began in 1990.19 As KD prevalence and incidence varied in the different periods, surveillance methods have been adjusted four times. However, there are a number of reasons that not all the results of the national KD surveillance can be used for assessing KD elimination. Firstly, KD surveillance was not able to provide the KD prevalence rate for all (every) endemic counties and townships (the smallest administrative unit). Secondly, KD surveillance obviously could not identify all KD cases because it was active surveillance which is a sampling survey of a very small number of the villages, not a population based surveillance, and latent KD cases are subclinical. Thirdly, KD surveillance was not fully comprehensive, mainly including the prevalence of KD. KD surveillance did not include the etiology or risk, i.e., selenium in some years, and the interventions taken in most years. The method developed in this study can overcome these limitations or shortcomings of the KD surveillance and also greatly reduce the workload so it was a small scale survey in comparison with passive surveillance, a whole population based surveillance.
The method for searching cases of chronic KD is equivalent to conducting a census. The suspected cases were found by village doctors and by case-searching in the county and township hospitals. Because village doctors were recruited locally and served their own villages, they were highly aware of the health conditions of the residents living in the villages.20 Collecting the data of suspected KD cases by the village doctors almost guaranteed that there were no missed cases with cardiomyopathies or cardiovascular diseases, and confirming KD cases by the medical teams of this study almost guaranteed the accuracy of the diagnosis. These ensured the reliability and accuracy of the data of the chronic KD cases.
The prevalence of latent KD was obtained by the key village survey, a non-probability survey. The selection of the key village was critical. The village of Xiangqianjin had the highest prevalence rate of KD in Yuanbao township in 2012 and the present study so this village was selected as the key village. The acute, subacute and chronic KD cases are clinical patients with severe signs and symptoms. However, the patients with latent KD do not see doctors because they are asymptomatic and subclinical and have reasonably good heart function (NYHA class I). The proportion of latent KD is the largest in the all types of KD, similar to the iceberg phenomenon. Active surveillance in the endemic areas of KD is the only way to identify latent KD cases. We can find the average prevalence of KD and its confidence interval with probability sampling, but cannot find the villages with the worst prevalence status. However, we cannot survey all people living in Yuanbao township because of the large workload. The key village was used to represent the highest prevalence rate of latent KD in Yuanbao township. If the prevalence of latent KD of the residents living in this village reached the KD elimination criteria, the probability of the prevalence rate of latent KD among the residents living in the township not reaching the criteria of KD elimination would be small. So we would regard that the prevalence of latent KD in Yuanbao township has reached the criteria of KD elimination. In addition to reducing the workload, another advantage of the key village survey is the high feasibility in comparison with probability sampling.
The information on KD intervention taken, the endemic scope and the population were collected by questionnaire survey of the professional staff of the Shangzhi County CDC, township doctors and village doctors, respectively. The respondents were extremely aware of the details of KD prevention and control work. All these not only ensured the reliability and accuracy of the data we collected but also could be completed in a timely and simple way.21,22
The head hair selenium level in Yuanbao township and the minimum head hair selenium level characteristic of populations in the non-endemic areas were not statistically significant, and higher than the max head hair selenium level in the endemic areas. However, there were 12 individuals (24%) with hair selenium level less than 0.12 mg/kg. This finding means that selenium deficiency still exists in the endemic areas. It is necessary to strengthen the dietary intake of selenium for people living in endemic areas of KD although the level of head hair selenium is not an indicator of the criteria of KD elimination.23
Innovation and limitations
This is the first study to explore the assessment of KD elimination and a case of translational epidemiology in the areas of disease surveillance and assessment of disease elimination.24,25 The need for assessment of KD elimination drove us to develop a method of assessment of KD elimination, which will be helpful to guide the practice of KD elimination assessment in larger endemic areas, i.e., at the levels of county, province and nation. The major limitation of this study is that the prevalence of latent KD among the residents living in Yuanbao township was represented by the result of the key village survey, which is not probability sampling, and has the risk of over estimating the prevalence status of latent KD.
Conclusions
The small-scale survey methodology we developed for assessing KD elimination at the township level was feasible. KD among the people living in Yuanbao township has not been eliminated. Further research on the proposed method should be at the county and province levels.
Authors' contributions: TW and QL conceived the study. SEL and CY analyzed and interpreted the data. SEL, QL and TW drafted the manuscript and revised the manuscript for intellectual content. All the authors implemented data acquisition. All authors read and approved the final manuscript. TW is guarantor of the paper.
Acknowledgments: We sincerely appreciate the Shangzhi county CDC and Yuanbao township hospital for assisting in completing the field work and all village doctors for collecting the data.
Funding: The study is supported by projects of the National Natural Science Foundation of China [H2401-81372938, H2401-81202154].
Competing interests: None declared.
Ethical approval: This study was carried out after getting ethical approval from the Ethical Review Board of Harbin Medical University.

{kind=link}
{kind=link}
Comments