





Objectives A systematic review and meta-analysis was conducted to investigate associations between family functioning and child adjustment (patient/siblings) after pediatric cancer diagnosis. Methods Database searches were performed using Web of Science, Pubmed, Cochrane, PsycInfo, and Embase. After screening 5,563 articles, 35 were identified regarding this topic; 30 contributed data for meta-analyses. Pearson’s r correlations were the effect of interest. Omnibus and family functioning domain-specific random-effects meta-analyses were conducted. Data are depicted in forest plots. Results A statistically significant association was found between family functioning and child adjustment (patient/siblings) after cancer diagnosis (r = 0.19; 95% CI: 0.13–0.24). Greater family cohesion, expressiveness, and support and less family conflict were each associated with better child adjustment outcomes. Conclusions Family functioning is associated with patient and sibling adjustment after pediatric cancer diagnosis. Limitations in the existing literature preclude strong conclusions about the size of these effects and potential moderators.
Pediatric cancer is a highly stressful experience that can challenge the whole family system, as well as the adjustment of the child receiving the diagnosis and other children within the family (Alderfer & Kazak, 2006). While there is evidence that most patients adjust well, some may experience social or emotional problems during (Kestler & LoBiondo-Wood, 2012) or after treatment (Kazak et al., 2001). Similarly, while most siblings adjust with time, some siblings show elevated levels of posttraumatic stress symptoms, negative emotional reactions, and poor quality of life when compared to norms or control groups (Alderfer et al., 2010). To optimize interventions for the children who experience difficulty, it is important to better understand factors that influence their adjustment.
The way in which the family as a whole responds to pediatric cancer is generally assumed to impact the adjustment of children within the family. Indeed, when faced with childhood cancer, families need to deal with intense emotions, communicate effectively, and renegotiate roles and responsibilities to accommodate the demands of treatment (Kazak et al., 2004; Marcus, 2012). While most families are resilient to these challenges (Van Schoors et al., 2015), children in poorly functioning families who struggle with these demands may be at greater risk for adjustment problems (e.g., Long, Marsland, & Alderfer, 2013; Myers et al., 2014).
This key principle is embedded within various family-systems models often applied to chronic illness populations. For example, the Social Ecology Model (Bronfenbrenner, 1977) illustrates how the child is nested within and influenced by the family system in addition to other social systems. The Double ABCX-Model (McCubbin et al., 1980), the Disability-Stress-Coping Model (Wallander & Varni, 1998), and the Family Adjustment and Adaptation Response Model (FAAR; Patterson, 2002) each propose that aspects of family functioning can be risk or protective factors for individual adjustment to illness or disability. Additionally, the Circumplex Model (Olson & Gorall, 2003), the Adolescence Resilience Model (Haase, 2004), the Process Model of Stress and Coping (Armstrong, Birnie-Lefcovitch, & Ungar, 2005), and the Family Resilience Process model (Walsh, 2002, 2003) each propose specific aspects of general family functioning that impact child adjustment such as family cohesion, conflict, adaptability, belief system, communication, organizational patterns, problem-solving ability, and social support.
While various reviews have summarized the impact of pediatric cancer on family functioning and/or child adjustment (Alderfer et al., 2010; Long & Marsland, 2011; Pai et al., 2007; Van Schoors et al., 2015), to date, there are no known systematic reviews or meta-analyses that summarize the empirical evidence investigating associations between family functioning and child adjustment to pediatric cancer. The primary aim of this paper is to fill that gap by providing an analysis, summary, and commentary on the current evidence regarding associations between the functioning of the family as a whole and child adjustment to pediatric cancer.
Method
This review is part of a series of systematic reviews of family functioning after childhood cancer (Van Schoors et al., 2015), sharing a single search strategy and following strict scientific methodology (Eiser, Hill, & Vance, 2000; Higgins & Green, 2011).
Literature Search and Inclusion Criteria
Literature searches in Web of Science, Pubmed, PsycInfo, Cochrane, and Embase were undertaken using the following search terms: (cancer OR tumor OR malignancy OR oncolog*) AND (child* OR pediatric) AND (family OR parental), AND (psycholog* OR adaptation OR adjustment). Studies selected for analysis examined associations between constructs capturing the functioning of the family as a whole (e.g., cohesion, flexibility, conflict, communication) and child (patient, sibling) adjustment (e.g., behavioral problems, anxiety, depression, psychosocial quality of life, posttraumatic stress) after cancer diagnosis. To maintain a focus on the family as a whole, studies examining parent–child relationship variables were not included. Eligible studies were quantitative, written in English, empirical (i.e., no reviews, case reports, commentaries, books, practice guidelines, conference abstracts, and dissertations), and involved families of children diagnosed with any type of cancer before age 18. Studies focused upon distress related to a medical procedure or appointment and those involving bereaved families were excluded, as these experiences are different from general adjustment to cancer diagnosis and treatment.
Study Selection
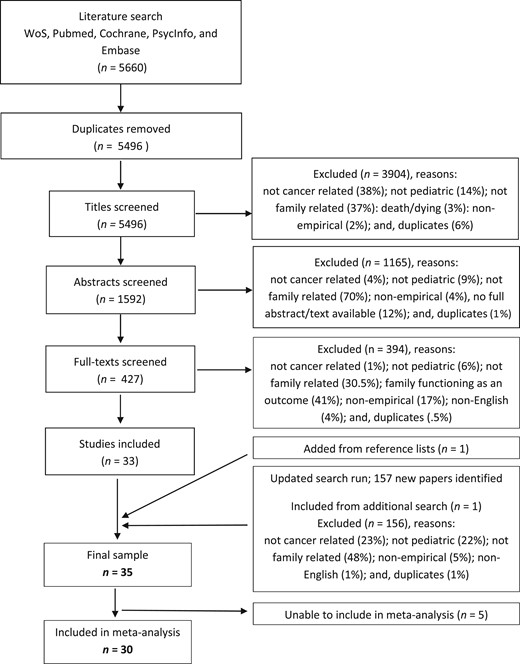
Steps in the search process.
Data Extraction
Data extraction was conducted in a systematic and standardized way, summarizing basic study information (e.g., year of publication, target population: patients/siblings, family functioning and adjustment variables assessed), theoretical framework, aspects of methodology, and general findings on abstraction sheets (available upon request). In addition, quantitative data were collected for the purpose of the meta-analysis, specifically sample size and bivariate correlations between family functioning and child adjustment variables or group sample size, means, standard deviations, and statistical data comparing independent groups (e.g., adjustment of children in “enmeshed” vs. “balanced” families). Contact was attempted with the authors of 17 papers to gather missing statistical data. Three author groups provided information, eight indicated that they no longer had access to the relevant data, three author groups did not respond, and valid contact information was unavailable for the authors of the remaining three studies. The last author checked all information extracted against original publications to ensure accuracy.
Quality Assessment
The first author rated the scientific merit and potential bias of each included study based upon the criteria published in Alderfer and colleagues (2010). This system evaluates nine aspects of quantitative studies (i.e., explicit scientific purpose, design and analysis appropriate to question posed, measurement reliability, statistical power and approach, internal and external validity, appropriate discussion, contribution to knowledge) on 3-point scales (1 = no or little evidence in fulfilling the criterion or low quality to 3 = good evidence or high quality). Individual aspect scores were averaged to obtain a total scientific merit score for each paper. The third author rated 33% of the included papers to assess reliability of the scientific merit evaluation. The single measure and average measures intraclass correlation coefficients across the two raters were .83 and .91, respectively, demonstrating good interrater reliability.
Data Analyses
The statistical information extracted from each study or provided by the authors was entered into Comprehensive Meta-Analysis (CMA) 3.0 statistical software (Borenstein, Hedges, Higgins, & Rothstein, 2015) for analysis. Group comparison results were converted to Pearson’s r (Lipsey & Wilson, 2001). The Pearson’s r values were transformed into Fisher’s Z correlations with calculation of the corresponding standard error for meta-analysis, then (back) transformed to Pearson’s r for interpretation and creation of forest plots. When authors indicated nonsignificant findings but did not provide statistical data, an effect size of 0 was used (Rosenthal, 1995). When authors indicated significant relationships without providing Pearson’s r or a specific p value, CMA was used to calculate the smallest possible statistically significant value for the sample size using a nondirectional test (Faul, Erdfelder, Lang, & Buchner, 2007).
The first level of analysis took an omnibus approach summarizing data across all domains of family functioning and all child outcomes. The sign of the correlation was standardized so that a positive value indicated that better family functioning (e.g., more communication, less conflict) was associated with better child adjustment (e.g., more social competence, fewer internalizing symptoms). A random-effects model meta-regression (method of moments) was used to account for nonnormally distributed effect sizes, and methodological heterogeneity across studies that could introduce significant random error (Borenstein et al., 2015; Cooper, 2017). Multiple effect sizes within studies/samples were averaged for this analysis. The Q statistic was used to assess heterogenity in the effect (Borenstein et al., 2015). To assess and adjust for the possibility of publication bias, funnel plots were created and the “trim and fill” algorithm (Duval & Tweedie, 2000) was used. To determine if combining patient and sibling data in this analysis was justified, child role (patient/sibling), a between-studies variable, was examined as a potential source of signficant heterogeneity in the analysis. The association between scientific merit rating and effect was also examined.
Because the omnibus analysis simply averaged effects within studies when multiple domains of family functioning were measured, subgroup meta-analyses were conducted to better estimate the size of associations between specific family functioning domains and child adjustment. These analyses were only conducted when at least five studies were available assessing a specific family functioning domain and when the number of estimated associations represented less than one-third of the available data in an effort to ensure reliability of the estimated effect (Valentine, Pigott, & Rothstein, 2010). Data are summarized in forest plots created with Microsoft Excel (Neyeloff, Fuchs, & Moreira, 2012).
Results
PART 1: General Characteristics of the Studies in the Review
The methods and findings of the 35 studies retained for this review are summarized in Supplementary Table 1. Most were cross-sectional (n = 27; 77%); only 23% (n = 8) were longitudinal. Sample size varied from 30 to 778 individuals, involving 30 to 389 families. The cancer-related time frame of these studies ranged from newly diagnosed families to those 30 years posttreatment. Leukemia, lymphoma, and brain tumors were the most frequently represented cancer diagnoses across studies. Patients were the focus of 28 of these studies.
The scientific merit ratings of the studies ranged from 1.39 to 2.67 on the 3-point scale used (Alderfer et al., 2010). Overall, the average quality rating across studies fell in the “good” range (M = 2.24), with four studies scoring below 2.0 (see Supplementary Table 1). The most common weaknesses across studies were the psychometric properties of the measures used (e.g., low internal consistency), internal validity (e.g., measuring predictor and outcome at same point in time), and external validity (e.g., poor enrollment rates, potentially biased samples limiting generalizability). Common strengths across studies included well-justified objectives and use of methods appropriate to address the stated study purpose.
Many aspects of family functioning have been examined in the literature as predictors of child adjustment after diagnosis of pediatric cancer, including cohesion/affective involvement/affective responsiveness, expressiveness/communication, conflict, adaptability, support, roles, problem-solving, control, organization, and overall family functioning. The most frequently investigated child adjustment outcomes included internalizing, externalizing, and total behavioral problems, posttraumatic stress, quality of life, and social competence.
Thirty of the 35 identified studies provided data for meta-analysis (Supplementary Table 1). One publication reported on two separate samples (Maurice-Stam et al., 2007), and these were treated as independent in analysis; data from two manuscripts reporting on the same sample (Ozono et al., 2007, 2010) were combined. Most studies reported multiple effects of interest (range: 1–45, M = 6.6, SD = 9.3) due to measurement of multiple family functioning domains, multiple forms of child adjustment, multiple reporters (parent, child) for single constructs, and multiple time points of assessment producing both cross-sectional and lagged associations. Five studies did not provide the statistical information needed to characterize bivariate associations between family functioning and child adjustment; three of these reported associations after adjusting for covariates (Barakat et al., 1997; Houtzager et al., 2004; Rait et al., 1992).
PART 2: General Association Between Family Functioning and Child Adjustment
Family Functioning and Child Outcomes—Omnibus Meta-Analysis
Across the 30 studies identified, 199 associations of interest were reported. A total of 22 associations were estimated within seven of these 30 studies. Significant heterogeneity beyond sampling error was apparent across studies within the omnibus meta-analysis, (Q [29] = 48.79, p = .012), validating the use of the random effects model. The summary estimate of the correlation between family functioning and child adjustment was 0.19, with a 95% confidence interval (95% CI) of 0.13 to 0.24. This value was significantly different from 0 (Z = 6.4, p < .0001); as family functioning improved, so did the adjustment of the child. Using a random-effects model, the trim and fill approach suggested that publication bias resulted in three missing effects; after imputation of these missing data, the coefficient was 0.16 (95% CI: 0.10–0.22).
Child Role
Child role (patient/sibling) was not a significant contributor to the heterogeneity observed across the summarized studies (Q [1] = 2.20, p = .14). The summary estimate of the correlation within studies (k = 24) investigating patient adjustment (0.16, 95% CI: 0.10–0.23) was not significantly different from the summary estimate of the correlation within studies (k = 6) investigating sibling adjustment (0.26, 95% CI: 0.15–0.38). Significant heterogeneity was present among the studies investigating patients (Q [23] = 37.88, p < .03), but not siblings (Q [5] = 7.68, p = .18). Using a random-effects model, the trim and fill approach suggested no publication bias among the patient studies, but that two sibling studies were probably missing. After imputation the sibling coefficient was 0.20 (95% CI: 0.08–0.32).
Scientific Merit
Meta-regression indicated that the size of the association was significantly related to the scientific merit of the study (Q [1] = 4.91, p < .03). As scientific merit improved, the size of the association between family functioning and child adjustment got smaller (−0.25, 95% CI: −0.48 to −0.03). Scientific merit accounted for 8% of the variance in effects (ΔI2 = .082) and significant heterogeneity remained (Q [27] = 40.86, p < .05).
PART 3: Specific Family Functioning Domains and Child Adjustment
Five family functioning domains were investigated in five or more studies: cohesion, expressiveness/communication, conflict, adaptability, and support. The adaptability meta-analysis was not conducted because 4 of 11 data points required estimation. Results for each of the remaining domains are presented below.
Cohesion
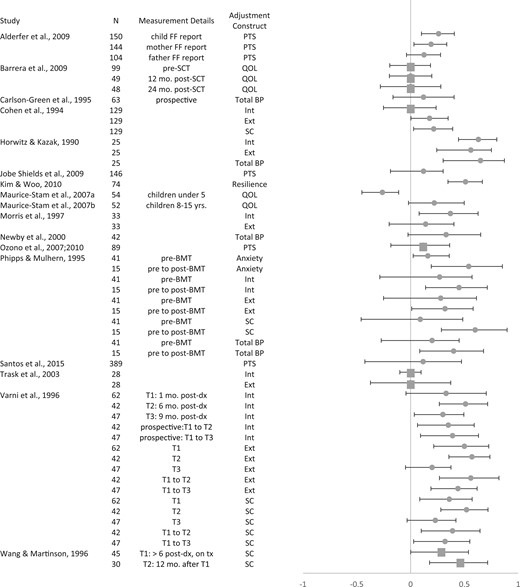
Forest plot: cohesion and child adjustment.
Note: Int = Internalizing Symptoms; Ext = Externalizing Symptoms; PTS = Posttraumatic Stress; QOL = Quality of Life; Total BP = Total Behavioral Problems; SC = Social Competence; FF = Family Functioning; BMT = Bone Marrow Transplant; SCT = Stem Cell Transplant; mo. = months; yrs. = years; dx = cancer diagnosis; tx = cancer treatment. Positive correlations indicate that more cohesion is associated with better child adjustment. Estimated effect sizes are depicted as squares.
Across adjustment outcomes, greater cohesion was significantly associated with better child adjustment (0.20, 95% CI: 0.11–0.29; Z = 4.32, p < .0001). There was, however, significant heterogeneity in the effect across studies (Q[16] = 37.93, p = .002). The trim and fill analysis indicated that three studies needed to be imputed to account for probable publication bias. The adjusted association was estimated as 0.14 (95% CI: .04–.24).
Expressiveness/Communication
Communication or expressiveness can be defined as the interchange of thoughts, feelings, experiences, and information within the family (Olson, 2000). This construct was addressed in 10 of the 30 studies in the omnibus meta-analysis, producing 42 associations of interest; five of these originating from two studies were estimated. Child adjustment outcomes assessed across these studies included internalizing and externalizing symptoms, posttraumatic stress, total behavioral problems, social competence, and anxiety.
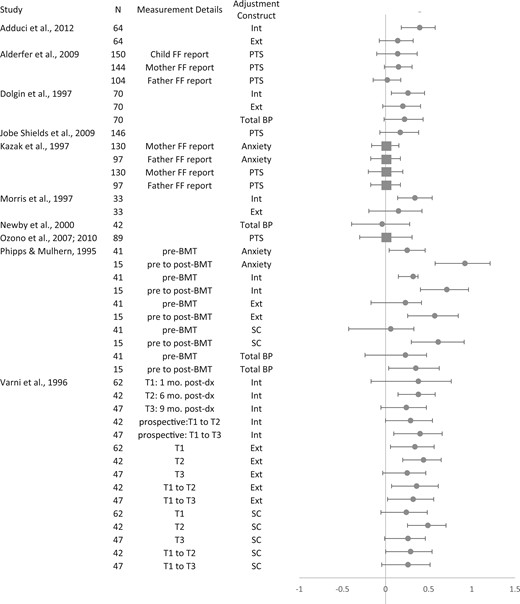
Forest plot: expressivity and child adjustment.
Note: Int = Internalizing Symptoms; Ext = Externalizing Symptoms; PTS = Posttraumatic Stress; Total BP = Total Behavioral Problems; SC = Social Competence; FF = Family Functioning; BMT = Bone Marrow Transplant; mo. = months; dx = cancer diagnosis. Positive correlations indicate that more expressivity/better communication is associated with better child adjustment.
Conflict
Conflict within the family can be defined as openly expressed anger and discord among family members (Moos & Moos, 1994). Associations between family conflict and child adjustment after cancer were examined in seven of the 30 studies included in the omnibus analysis and 33 associations of interest; none were estimated. Adjustment outcomes assessed in these studies included internalizing and externalizing symptoms, posttraumatic stress, total behavioral problems, social competence, and anxiety.
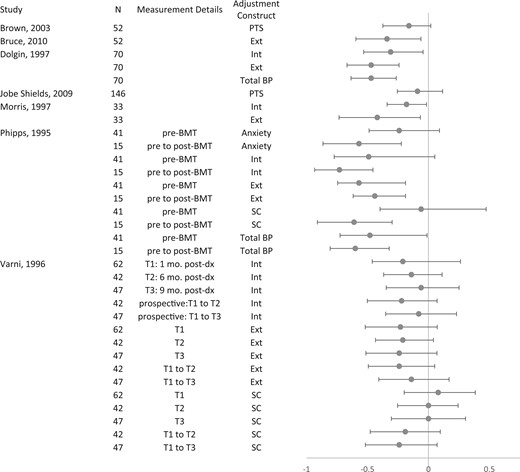
Forest plot: conflict and child adjustment.
Note: Int = Internalizing Symptoms; Ext = Externalizing Symptoms; PTS = Posttraumatic Stress; Total BP = Total Behavioral Problems; SC = Social Competence. Negative correlations indicate that greater conflict is associated with poorer child adjustment.
Family Support
Family support refers to practical assistance and encouragement and caring from the family received or perceived by an individual (Walsh, 2002). This construct was assessed in six of the 30 studies in the omnibus analysis, providing 18 associations of interest; two of which arising from a single study were estimated. Across these studies, child adjustment outcomes included internalizing and externalizing symptoms, total behavioral problems, anxiety, depression, posttraumatic stress, negative affect, and social competence.
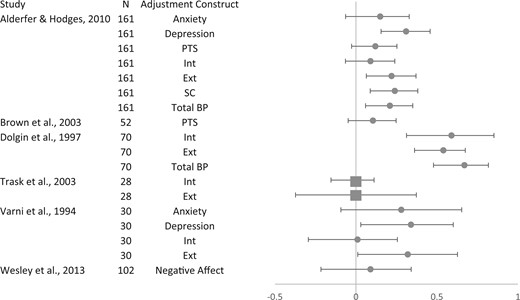
Forest plot: support and child adjustment.
Note: Int = Internalizing Symptoms; Ext = Externalizing Symptoms; PTS = Posttraumatic Stress; Total BP = Total Behavioral Problems; SC = Social Competence; FF = Family Functioning; BMT = Bone Marrow Transplant; mo. = months; dx = cancer diagnosis. Positive correlations indicate that more support is associated with better child adjustment. Estimated effect sizes are depicted as squares.
Discussion
To our knowledge, this is the first meta-analysis investigating associations between family functioning and child adjustment after pediatric cancer diagnosis. The results of our meta-analysis generally indicate that better family functioning and specifically greater family cohesion, support, and expressiveness and less family conflict are associated with better child adjustment. These general finding are consistent across patients and siblings. The evidence, however, is not overwhelming, and the sizes of the summary correlations are not large. As such, our conclusions are tentative and not without qualifications. Below, we address the quality and limitations of the current literature and our analysis, provide recommendations for further research, and discuss clinical considerations.
Quality and Limitations of the Current Literature and Our Analyses
The scientific merit of the included studies ranged from poor to exceptional, with the average rating across all studies falling slightly above the mid-point on the scale (Alderfer et al., 2010). In these individual studies, the most commonly noted weakness included small, heterogeneous samples characterized by a broad range of diagnoses, child ages, and time since cancer diagnosis or treatment. Furthermore, the psychometric properties of the measures used to assess family functioning were sometimes a concern (e.g., low internal consistencies) and threats to both internal and external validity were apparent.
Meta-analysis was applied to the results of these studies to attempt to pool the data and circumvent problems with small sample sizes and heterogeneous samples. The benefits of using meta-analysis are discussed in more length by Valentine, Pigott, and Rothstein (2010) and Cooper (2017), including the ability to go beyond tallying significant and nonsignificant findings by estimating confidence intervals for effect sizes across studies. However, the limitations of this method also need to be appreciated. The studies summarized here were heterogeneous in regard to design (i.e., cross-sectional, prospective) and specific family functioning and child outcomes assessed—distinctions that are theoretically and empirically important, but were lost in the omnibus analysis. Dependencies in the data precluded analyses to determine whether specific family functioning domain and specific child adjustment outcome accounted for significant heterogeneity in the associations found and to determine the relative strength of associations between various family functioning domains and various child adjustment outcomes.
It should be noted that our method of estimating associations when statistical data were not provided was conservative and likely led to underestimation of the association, but this is preferable to introducing bias by ignoring null or incompletely reported results (Rosenthal, 1995). Further, our analysis demonstrated that associations between family functioning and child adjustment were larger in studies with poorer scientific merit. This likely reflects bias in our publication practices. While well-designed studies are likely to be published regardless of results, more poorly designed studies may only be published when large, significant effects are reported. Statistical adjustments were made as needed within analyses to offset likely publication bias.
Additionally, it should be noted that the associations between family functioning and child adjustment uncovered in our analyses are specific to families of children with cancer. These findings may or may not generalize to other illness populations, and it is unclear whether these associations are similar to those for typically developing children in the general population. While our analysis only focused upon the functioning of the family as a whole, associations between parent–child relationships variables and child adjustment should be investigated.
Recommendations for Future Research
Theory should underlie the design of research and our research should aim to refine theory. One example of the lack of attention to this issue emerges in studies that acknowledge that, in theory, both high and low levels of certain family functioning variables are problematic, but then use research designs and statistical techniques based upon linear instead of curvilinear models. Second, attention needs to be paid to the conceptualization and measurement of family functioning constructs. Some measures of family functioning have low internal consistency in pediatric populations. Further, a small group of measures (e.g., Family Environment Scale [FES], Family Adaptability and Cohesion Scale [FACES]) are typically used. Aspects of family functioning that could uniquely promote resilience for children facing cancer (e.g., managing strong emotions, experiencing and expressing gratitude, repairing relationship rifts) may therefore go unexamined. Third, more research into the associations between family functioning and child adjustment is needed. Many of the studies uncovered were from the past century. These data may not reflect current patterns, leaving important questions unanswered. Future research should include more homogenous or larger sample sizes, potentially through multi-site studies, to draw stronger conclusions regarding the associations between family functioning and child adjustment in specific contexts or to systematically investigate the role of moderators or mediators. For example, certain aspects of family functioning may be more important to child adjustment at certain time points (e.g., near diagnosis, coming off treatment), for those with specific biological risk profiles (e.g., central nervous system disease), during different developmental stages, or for families embedded in different cultures. Comparing associations between family functioning and child adjustment across populations (e.g., illness and nonillness groups) would also be informative. Lastly, basic statistical information needs to be published in individual studies to support future meta-analyses including the values of all significant and nonsignificant statistical analyses and associations between constructs.
Clinical Considerations
Most children adapt well after pediatric cancer, although an important subset experiences problems (Alderfer et al., 2010; Kestler & LoBiondo-Wood 2012). The results of this meta-analysis indicate that better family functioning supports child adjustment. Therefore, we recommend assessing the unmet needs and providing support to all family members and the family as a whole when a child is diagnosed with cancer. Difficulties in the way in which the family is functioning after pediatric cancer may, indeed, have implications for the adjustment of all individuals within the family, and interventions at the level of the family may serve to help ameliorate or prevent adjustment problems for all children. A universal preventative model integrating screening and identifying risk and protective factors (Kazak et al., 2001) across the family may be most efficient and support long-term wellness. Indeed, focusing on building the family’s strengths such as their emotional bonds with one another, ability to communicate openly, and resolve conflict may promote child adjustment while fostering family resiliency and growth.
Supplementary Data
Supplementary data can be found at: http://www.jpepsy.oxfordjournals.org/.
Acknowledgements
Special thanks to Diane Fairclough, DrPH, MSPH., for her guidance regarding statistical analysis of the data.
Funding
Conflicts of interest: None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}