





Abstract
Neurological soft signs (NSS) are related to grey matter and functional brain abnormalities in schizophrenia. Studies in healthy subjects suggest, that NSS are also linked to white matter. However, the association between NSS and white matter abnormalities in schizophrenia remains to be elucidated. The present study investigated, if NSS are related to white matter alterations in patients with schizophrenia. The total sample included 42 healthy controls and 41 patients with schizophrenia. We used the Neurological Evaluation Scale (NES), and we acquired diffusion weighted magnetic resonance imaging to assess white matter on a voxel-wise between subject statistic. In patients with schizophrenia, linear associations between NES with fractional anisotropy (FA), radial, axial, and mean diffusivity were analyzed with tract-based spatial statistics while controlling for age, medication dose, the severity of the disease, and motion. The main pattern of results in patients showed a positive association of NES with all diffusion measures except FA in important motor pathways: the corticospinal tract, internal capsule, superior longitudinal fascicle, thalamocortical radiations and corpus callosum. In addition, exploratory tractography analysis revealed an association of the right aslant with NES in patients. These results suggest that specific white matter alterations, that is, increased diffusivity might contribute to NSS in patients with schizophrenia.
Introduction
Neurological soft signs (NSS) are subtle motor and sensory deficits, including motor coordination, sequencing of complex motor tasks, and sensory integration.1 NSS have been considered to indicate neurodevelopmental delay typically improving during adolescence, but persisting in a variety of mental disorders, best documented in schizophrenia and subjects at risk for psychosis.2,3 NSS frequency increases along a continuum of risk for psychosis, from healthy subjects to first-degree relatives to subjects at risk and patients with psychosis.2–7 In patients with schizophrenia, NSS are related to negative and positive symptoms,4 auditory verbal hallucinations,8 cognitive deficits,4,9 social functioning,10 duration of illness9, and predict poor treatment outcome.11,12 Collectively, NSS are linked to the risk of psychosis as well as to the core features of schizophrenia spectrum disorders.
NSS are thought to arise from aberrant neural maturation and brain connectivity. Motor and sensory functions tested in NSS examinations require a complex interplay of multiple extended brain networks spanning the fronto-parietal cortices, basal ganglia, thalamus, and cerebellum.13–15 In healthy subjects, neurodevelopmental markers of fronto-temporal brain morphology correlated with NSS in adulthood.16 Similarly, multiple reports linked NSS severity to morphological markers of aberrant brain maturation in fronto-parietal brain areas in schizophrenia.17–19 These findings are largely consistent with previous work associating NSS with reduced grey matter volumes in pre- and postcentral gyrus, dorsolateral prefrontal cortex, basal ganglia, thalamus, and cerebellum in patients with psychosis.13,20–24 Importantly, most of the associations between morphological alterations and NSS were detected in an extended motor network comprising the cortico-cerebellar-thalamo-cortical-circuit. Indeed, resting state functional connectivity indicates that NSS severity is associated with poor fronto-cerebellar or fronto-parietal connectivity.25,26 However, connectivity between distant brain areas heavily relies on structural connectivity of white matter (WM) pathways. Still, studies linking NSS with white matter microstructure are scarce and limited to healthy subjects.27
Aberrant white matter properties have become a standard finding of group comparisons in psychosis, typically with decreased fractional anisotropy and increased diffusivity.28–33 Some of the major white matter tracts such as the superior longitudinal fascicle (SLF) show declining white matter properties with age in schizophrenia, while studies also suggest abnormal neural maturation in these tracts in subjects at risk for psychosis.28,33,34
The maturation of white matter motor tracts starts in the second and third trimester in utero and progresses until early adulthood in humans.35,36 Furthermore, the acquisition of motor skills throughout childhood has been linked to white matter maturation of major motor tracts, such as the corpus callosum or corticospinal tract (CST).37,38 Therefore, subtle alterations of motor function such as NSS in adults with schizophrenia spectrum disorders could be associated with typical alterations of white matter microstructure in psychosis, given that delayed neural maturation could be the common denominator of both phenomena. In fact, NSS indicated aberrant cerebellar-thalamic tract development in subjects at risk for psychosis.39
In sum, NSS and schizophrenia are both considered to have neurodevelopmental origins and to include behaviors attributed to dysconnectivity between distant brain areas.40–43 Therefore, researchers have begun to view motor abnormalities broadly and NSS specifically as a window to study aberrant neural maturation in schizophrenia.3,44,45 In addition to the above-mentioned studies on NSS and grey matter morphology, the field should also consider structural connectivity in the white matter to understand variance in NSS in psychosis.
The aim of our study was to investigate the association between NSS and white matter alterations in adults with schizophrenia. White matter alterations are most commonly investigated with fractional anisotropy (FA) or mean diffusivity (MD), which are composites of different WM parameters. While FA and MD are conventionally reported, other WM parameters may disclose biologically relevant complementary information. Animal models suggest that radial diffusivity (RD) indicates demyelination, while axial diffusivity (AD) indicates axonal degeneration.46,47 In fact, RD and AD have been associated with schizophrenia pathology or psychosis dimensions.48–51 Furthermore, a study in healthy subjects detected associations between RD in the corpus callosum and NSS.27 Since patients with schizophrenia present NSS more often than healthy controls3,4 and concurrently show white matter abnormalities,29 we hypothesize associations between NSS severity and increased diffusivity (particularly increased RD and MD), but decreased FA in several white matter regions of the motor system, including the corpus callosum, internal capsule, SLF, and CST in patients with schizophrenia. Finally, we apply a tractography approach to specifically explore associations of NSS with FA of three important motor tracts: CST, SLF, and the aslant tract.
Methods
Participants
Forty-seven patients with schizophrenia and 44 healthy controls were enrolled in the study. Six patients and two controls had to be excluded from the whole-brain analyses due to poor diffusion image quality. For the exploratory tractography analysis, we excluded 4 patients due to artefacts in the fiber tracts of interest. Thus, 41 patients with schizophrenia (77.5%), schizophreniform (17.5%), and schizoaffective disorders (5%) and 42 matched healthy controls were included for the main analyses. Patients were recruited from the University Hospital of Psychiatry and Psychotherapy Bern, Switzerland, and all healthy controls via advertisement or among staff. The groups were matched for sex, age, and education. All subjects were right-handed as evaluated by the Edinburgh Handedness Inventory.52 The study was performed in accordance with the Declaration of Helsinki and approved by the local ethics committee in Bern (KEK-BE 025/13). All participants gave written informed consent.
Patients were diagnosed using the Mini-International Neuropsychiatric Interview according to criteria of the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5). Further assessments included the Comprehensive Assessment of Symptoms and History,53,54 the Positive and Negative Syndrome Scale (PANSS),55 and the Neurological Evaluation Scale (NES)56 to assess NSS. Most patients (90%) currently received antipsychotic treatment. Dosages were quantified as the average chlorpromazine equivalents (CPZ) per day.57 Demographic and clinical characteristics of all subjects are provided in Table 1.
Demographic and Clinical Characteristics
| Statistics | ||||
|---|---|---|---|---|
| Variablesa | Controls (n = 42) | Patients (n = 41) | X2 | P |
| Sex (men/women) | 24/18 | 24/17 | .017 | .898 |
| Mean (SD) | Mean (SD) | t | p | |
| Age (years) | 39.3 (13.7) | 37.9 (11.6) | −.478 | .634 |
| Education (years) | 14.1 (2.7) | 13.7 (3.1) | −.743 | .460 |
| NES total | 3.7 (3.7) | 12.2 (10.9) | 4.74 | .001 |
| NES sensory integration | 1.1 (1.2) | 2.5 (2.6) | 2.98 | .004 |
| NES motor coordination | .6 (1.2) | 2.2 (2.6) | 3.52 | .001 |
| NES sequence | .9 (1.8) | 3.0 (2.9) | 3.89 | .001 |
| NES other | 1.0 (1.4) | 4.6 (4.6) | 4.77 | .001 |
| CPZ (mg) | 419.0 (362.9) | |||
| DOI (months) | 151.1 (152.3) | |||
| PANSS positive | 18.2 (6.3) | |||
| PANSS negative | 18.2 (5.2) | |||
| PANSS total | 71.7 (17.1) | |||
| Statistics | ||||
|---|---|---|---|---|
| Variablesa | Controls (n = 42) | Patients (n = 41) | X2 | P |
| Sex (men/women) | 24/18 | 24/17 | .017 | .898 |
| Mean (SD) | Mean (SD) | t | p | |
| Age (years) | 39.3 (13.7) | 37.9 (11.6) | −.478 | .634 |
| Education (years) | 14.1 (2.7) | 13.7 (3.1) | −.743 | .460 |
| NES total | 3.7 (3.7) | 12.2 (10.9) | 4.74 | .001 |
| NES sensory integration | 1.1 (1.2) | 2.5 (2.6) | 2.98 | .004 |
| NES motor coordination | .6 (1.2) | 2.2 (2.6) | 3.52 | .001 |
| NES sequence | .9 (1.8) | 3.0 (2.9) | 3.89 | .001 |
| NES other | 1.0 (1.4) | 4.6 (4.6) | 4.77 | .001 |
| CPZ (mg) | 419.0 (362.9) | |||
| DOI (months) | 151.1 (152.3) | |||
| PANSS positive | 18.2 (6.3) | |||
| PANSS negative | 18.2 (5.2) | |||
| PANSS total | 71.7 (17.1) | |||
aNES, Neurological Evaluation Scale; CPZ, average chlorpromazine equivalents; DOI, duration of illness; PANSS, Positive and Negative Syndrome Scale.
Demographic and Clinical Characteristics
| Statistics | ||||
|---|---|---|---|---|
| Variablesa | Controls (n = 42) | Patients (n = 41) | X2 | P |
| Sex (men/women) | 24/18 | 24/17 | .017 | .898 |
| Mean (SD) | Mean (SD) | t | p | |
| Age (years) | 39.3 (13.7) | 37.9 (11.6) | −.478 | .634 |
| Education (years) | 14.1 (2.7) | 13.7 (3.1) | −.743 | .460 |
| NES total | 3.7 (3.7) | 12.2 (10.9) | 4.74 | .001 |
| NES sensory integration | 1.1 (1.2) | 2.5 (2.6) | 2.98 | .004 |
| NES motor coordination | .6 (1.2) | 2.2 (2.6) | 3.52 | .001 |
| NES sequence | .9 (1.8) | 3.0 (2.9) | 3.89 | .001 |
| NES other | 1.0 (1.4) | 4.6 (4.6) | 4.77 | .001 |
| CPZ (mg) | 419.0 (362.9) | |||
| DOI (months) | 151.1 (152.3) | |||
| PANSS positive | 18.2 (6.3) | |||
| PANSS negative | 18.2 (5.2) | |||
| PANSS total | 71.7 (17.1) | |||
| Statistics | ||||
|---|---|---|---|---|
| Variablesa | Controls (n = 42) | Patients (n = 41) | X2 | P |
| Sex (men/women) | 24/18 | 24/17 | .017 | .898 |
| Mean (SD) | Mean (SD) | t | p | |
| Age (years) | 39.3 (13.7) | 37.9 (11.6) | −.478 | .634 |
| Education (years) | 14.1 (2.7) | 13.7 (3.1) | −.743 | .460 |
| NES total | 3.7 (3.7) | 12.2 (10.9) | 4.74 | .001 |
| NES sensory integration | 1.1 (1.2) | 2.5 (2.6) | 2.98 | .004 |
| NES motor coordination | .6 (1.2) | 2.2 (2.6) | 3.52 | .001 |
| NES sequence | .9 (1.8) | 3.0 (2.9) | 3.89 | .001 |
| NES other | 1.0 (1.4) | 4.6 (4.6) | 4.77 | .001 |
| CPZ (mg) | 419.0 (362.9) | |||
| DOI (months) | 151.1 (152.3) | |||
| PANSS positive | 18.2 (6.3) | |||
| PANSS negative | 18.2 (5.2) | |||
| PANSS total | 71.7 (17.1) | |||
aNES, Neurological Evaluation Scale; CPZ, average chlorpromazine equivalents; DOI, duration of illness; PANSS, Positive and Negative Syndrome Scale.
Exclusion criteria contained substance abuse or dependence (except nicotine), current or past neurological or medical conditions related to motor impairments or WM abnormalities (e.g. stroke, multiple sclerosis, dystonia, idiopathic Parkinson’s syndrome, polyneuropathy, neoplasms), and head trauma with loss of consciousness or electroconvulsive treatment. Further, we excluded participants with any contraindications to magnetic resonance imaging (MRI) scans (e.g. metallic implants, pregnancy and claustrophobia). Additional exclusion criteria for healthy controls were a history of any psychiatric diagnosis and any first-degree relatives with schizophrenia spectrum disorders.
Neurological Evaluation Scale (NES)
The NES is a structured clinical examination to assess the neurological impairment in schizophrenia.56 The scale consists of 26 items and is divided into four subscales: sensory integration, motor coordination, sequencing of complex motor acts, and “others.” Sensory integration includes items like audiovisual integration, bilateral extinction, graphesthesia, right-left confusion, and stereognosis. The subscale motor coordination encompasses dysdiadochokinesis (rapid alternating movements), finger to thumb opposition, finger to nose test, and tandem walk. The subscale sequencing of complex motor acts comprises the fist-edge-palm test, fist-ring test, Ozeretski test, and rhythm tapping test. The subscale “others” includes the assessment of hemispheric dominance, eye movement deficits, frontal release signs, and short-term memory. Each item can be scored on a 3-point scale (0 = no abnormality, 1 = mild impairments, 2 = marked impairments).56 The NES shows high interrater reliability, high intraclass correlations for the total score and subscales and good internal consistency for patients with schizophrenia and healthy controls.58 It is further related to cognitive function, positive and negative symptoms.58 NSS assessments were conducted by one rater (K.S.), who was intensively trained by the principal investigator to achieve κ ≥ .85 on all clinical and motor rating scales.
MRI Acquisition
For diffusion tensor imaging (DTI), a 3T MRI scanner (Siemens Magnetom Trio; Siemens Medical Solutions, Erlangen, Germany) with a 12-channel radio frequency headcoil was used. We applied a spin echo planar imaging sequence (59 slices, FOV=256 × 256 mm2, sampled on a 128 × 128 matrix, slice thickness = 2 mm, gap between slices = 0 mm, resulting in 2 mm3 isotopic voxel resolution) covering the whole brain and a repetition time/echo time (TR/TE) = 8000/92 ms (40 mT/m gradient, 6/8 partial Fourier, GRAPPA acceleration factor 2, bandwidth 1346 Hz/pixel). Diffusion-weighted images (DWI) were measured along 42 directions applying a b-value = 1300 s/mm2 and were set in the axial plane parallel to the AC-PC line. We used a balanced and rotationally invariant diffusion-encoding scheme over the unit sphere to generate DTI data. Acquisition time was 6 min.
White Matter Analyses
DTI analyses were performed with the FMRIB (Functional Magnetic Resonance Imaging of the Brain’s diffusion toolbox) Software Library (FSL) (http://www.fmrib.ox.ac.uk/fsl), which comprises the Tract-Based Spatial Statistics (TBSS) software.59,60 The images were first corrected for head movements and eddy currents (using “eddy-correct” of FSL). A brain extraction tool (using “BET-tool” of FSL)61 and a tensor model were applied which resulted in the FA images (using “DTIFIT”). Next, the nonlinear registration aligned the FA data across subjects. In a post-registration step, the FA data were then aligned to a 1 mm3 Montreal Neurological Institute (MNI) standard space applying FMRIB’s Non-Linear Image Registration Tool,62,63 which uses a b-spline representation of the registration warp field.64 For the statistical analyses, a mean FA skeleton was created based on a thinned mean FA image. We applied a FA threshold of 0.2 to exclude non-skeletal voxels. The aligned FA data of each subject was projected onto the mean FA skeleton. Then, we performed voxel-wise between-subject statistics. In addition to FA images, AD, MD, and RD were estimated by fitting a tensor model to the data at each voxel. We applied the nonlinear warps and skeleton projection of the FA images to MD, RD, and AD images using the “non_fa” option. To further correct for motion, we calculated framewise displacement according to Power and colleagues65 using “topup” in FSL. The method of the tractography is provided in the supplementary material.
Statistical Analysis
All statistical analyses for behavioral data were computed with IBM SPSS version 26 or Matlab version 2017a. Demographic and clinical data were compared using a chi-square test or independent t-tests in SPSS. Statistical analyses for WM were computed with TBSS, which uses a non-parametric approach including permutation test theory with a general linear model (GLM) design matrix.60 First, in order to describe the white matter alterations in our sample we calculated group differences in diffusion measures (FA, MD, AD, RD) with the covariates age and motion index.65 A randomize tool66 (5000 permutations) with a threshold-free cluster enhancement (TFCE) correction method67 tested the skeletonized FA, MD, RD, and AD group differences. The significant regions were labelled and located by mapping the corrected statistical map on the Johns Hopkins University (JHU)-ICBM-DTI-81 WM labels atlas and the JHU-WM tractography atlas in MNI space.68,69 Only clusters exceeding 50 voxels per WM region were included.
Second, in the main analyses we examined the voxel-wise linear association between NES total scores and FA, MD, RD, and AD within patients. Age, current medication dose, symptom severity (measured by the PANSS total) and motion65 were included as covariates of no interest and TFCE with 5’000 permutations was calculated. The TFCE corrected p-values were divided by four to apply Bonferroni correction for multiple comparisons, rendering P ≤ .0125 (FWE corrected) as significant. Third, in an explorative approach we calculated voxel-wise associations between the four WM parameters and three NES subscales within patients using the same covariates as for NES total. The TFCE corrected P-values of these exploratory analyses were not further corrected for multiple comparisons. Finally, for tractography, we calculated partial correlations across all patients and included age and medication dose as covariates. In detail, we calculated correlations for FA of the bilateral SLF, CST, and aslant tract with NES total score and subscales motor coordination, sensory integration, and sequence of complex motor tasks. These tractography analyses are exploratory and remain uncorrected for multiple comparisons.
Results
Behavioral and Clinical Data
Demographic and clinical characteristics of the participants are presented in table 1 and table S1 in the supplementary material. Patients with schizophrenia and healthy controls did not differ regarding sex, age, and education (P > .05). However, as expected, patients with schizophrenia showed more NSS. NES scores correlated positively with age, duration of illness, current dose of antipsychotics, negative symptom severity, as well as measures of dyskinesia, parkinsonism, and catatonia. However, none of the correlations would survive correction for multiple comparisons (see table S2 in the supplementary material).
Descriptive Group Differences in White Matter Parameters
This study also found the well-known alterations in white matter parameters in patients with schizophrenia compared to healthy subjects. In multiple white matter areas, patients had lower FA values compared to healthy controls (P ≤ .05, FWE corrected). The largest clusters of group differences appeared in the corpus callosum and anterior corona radiata, other areas included the internal and external capsule, inferior-fronto-occipital fascicle, inferior longitudinal fascicle, CST, and SLF (see supplementary Table S3. Patients had higher MD than controls in fewer and smaller clusters of WM compared to FA group differences, including the corpus callosum, internal and external capsule, corona radiata, SLF, and inferior fronto-occipital fasciculus (see supplementary Table S4). Moreover, patients with schizophrenia had higher RD values than controls in areas including the corpus callosum, corona radiata, internal and external capsule, inferior-fronto-occipital fascicle, inferior longitudinal fascicle, CST, and SLF (see supplementary Table S5). We found no differences in AD between patients and controls.
Associations of White Matter Markers With Neurological Soft Signs in Patients With Schizophrenia
We tested for linear relationships between the NES total score and four white matter diffusion measures: FA, AD, MD, and RD. We detected positive linear relationships for AD, MD, and RD with NES total scores. Hence, stronger NSS are linked to higher AD, MD and RD values in different white matter areas. In contrast, we failed to detect linear associations between NES total score and FA.
NES total score was positively associated with AD values in multiple white matter regions and motor pathways including the corpus callosum, internal and external capsule, corona radiata, thalamic radiation, CST, superior and inferior fronto-occipital fasciculus, inferior longitudinal fasciculus, and SLF (P ≤ .0125, FWE corrected) (see figure 1a, table 2a). Similarly, MD values were positively associated with NES total score in the same white matter regions, but some clusters were slightly smaller, especially in posterior brain regions (P ≤ .0125, FWE corrected) (see figure 1b, table 2b). Finally, NES total was positively related to RD values in frontal lobe clusters in the corpus callosum, corona radiata, and anterior thalamic radiation (P ≤ .0125, FWE corrected) (see figure 1c, table 2c). Of note, the clusters with associations in RD seem to spatially overlap with clusters depicting associations between NES and MD or AD. Likewise, many MD and NES associations share the locations of associations between AD and NES.
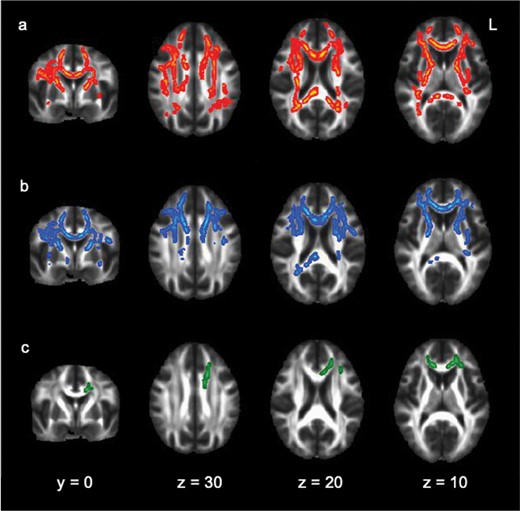
The TBSS image shows the linear relationships between NES total score and different parameters of white matter integrity: (a) axial diffusivity (b) mean diffusivity, (c) radial diffusivity. Significant clusters are thickened for visual purposes and are indicated in different colors at P < .05, FWE corrected, projected on a standardized diffusion-weighted image (FMRIB58_FA). Y and Z indicate the coordinates of the image slices in mm.
Location of Significant Linear Relationship Between NES total and (a) axial diffusivity, (b) mean diffusivity, (c) radial diffusivity in patients with schizophrenia
| Center of Gravity (mm Coordinates) | |||||
|---|---|---|---|---|---|
| X | Y | Z | Cluster Size | P(FWE-corr) | |
| (a) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 1.4 | 27.8 | 8.5 | 1372 | 0.003 |
| Body of corpus callosum | 1.4 | 1.4 | 25.7 | 1454 | 0.005 |
| Splenium of corpus callosum | 4.5 | −41.4 | 18.9 | 734 | 0.006 |
| Anterior limb of internal capsule R | 20.2 | 9.1 | 10.4 | 354 | 0.005 |
| Anterior limb of internal capsule L | −19.0 | 9.1 | 9.9 | 227 | 0.008 |
| Posterior limb of internal capsule R | 23.5 | −13.6 | 9.5 | 338 | 0.006 |
| Posterior limb of internal capsule L | −22.1 | −12.5 | 9.7 | 181 | 0.008 |
| Retrolenticular part of internal capsule R | 30.9 | −31.0 | 10.5 | 181 | 0.007 |
| Retrolenticular part of internal capsule L | −30.8 | −28.0 | 5.9 | 310 | 0.006 |
| Anterior corona radiata R | 23.3 | 25.8 | 10.1 | 906 | 0.005 |
| Anterior corona radiata L | −22.0 | 23.4 | 14.9 | 563 | 0.006 |
| Superior corona radiata R | 24.3 | −7.7 | 31.8 | 860 | 0.004 |
| Superior corona radiata L | −24.3 | −4.3 | 30.2 | 680 | 0.005 |
| Posterior corona radiata R | 24.9 | −37.7 | 28.3 | 316 | 0.006 |
| Posterior corona radiata L | −26.2 | −38.5 | 25.6 | 224 | 0.006 |
| Posterior thalamic radiation R | 33.0 | −50.0 | 13.9 | 189 | 0.008 |
| External capsule R | 29.2 | 0.7 | 3.7 | 199 | 0.007 |
| External capsule L | −31.7 | −8.9 | 4.7 | 415 | 0.006 |
| Superior fronto-occipital fasciculus R | 22.2 | 5.7 | 21.0 | 68 | 0.005 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −20.8 | 16.6 | 10.7 | 316 | 0.007 |
| Anterior thalamic radiation R | 20.2 | 14.2 | 9.3 | 248 | 0.005 |
| Corticospinal tract L | −23.3 | −21.9 | 31.3 | 298 | 0.006 |
| Corticospinal tract R | 23.8 | −21.4 | 28.0 | 474 | 0.005 |
| Inferior fronto-occipital fasciculus L | −31.0 | 10.0 | 1.8 | 370 | 0.006 |
| Inferior fronto-occipital fasciculus R | 27.8 | 30.8 | 5.0 | 365 | 0.005 |
| Inferior longitudinal fasciculus L | −42.6 | −21.4 | −9.2 | 73 | 0.007 |
| Superior longitudinal fasciculus L | −37.6 | −41.6 | 28.3 | 147 | 0.007 |
| Superior longitudinal fasciculus R | 36.8 | −23.5 | 31.8 | 476 | 0.006 |
| (b) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 1.0 | 27.8 | 8.6 | 1440 | 0.002 |
| Body of corpus callosum | −0.2 | 5.6 | 26.6 | 1332 | 0.004 |
| Splenium of corpus callosum | 13.7 | −41.6 | 20.4 | 283 | 0.012 |
| Anterior limb of internal capsule R | 20.3 | 9.8 | 9.9 | 328 | 0.005 |
| Anterior limb of internal capsule L | −18.4 | 8.8 | 9.2 | 312 | 0.005 |
| Posterior limb of internal capsule R | 21.1 | −5.5 | 10.9 | 56 | 0.007 |
| Retrolenticular part of internal capsule L | −32.3 | −28.8 | 4.8 | 188 | 0.010 |
| Anterior corona radiata R | 22.1 | 26.7 | 11.1 | 1155 | 0.004 |
| Anterior corona radiata L | −20.6 | 27.7 | 10.7 | 1012 | 0.004 |
| Superior corona radiata R | 23.5 | −0.8 | 31.9 | 607 | 0.005 |
| Superior corona radiata L | −22.5 | −2.3 | 31.7 | 513 | 0.005 |
| Posterior corona radiata R | 22.2 | −41.0 | 32.0 | 120 | 0.012 |
| Sagittal stratum L | −40.0 | −30.5 | −9.1 | 124 | 0.010 |
| External capsule R | 29.7 | 9.1 | −1.6 | 314 | 0.005 |
| External capsule L | −30.3 | −1.3 | 0.0 | 574 | 0.008 |
| Superior fronto-occipital fasciculus R | 22.2 | 5.6 | 21.2 | 64 | 0.004 |
| Superior fronto-occipital fasciculus L | −21.1 | 5.1 | 20.1 | 54 | 0.005 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −20.1 | 17.0 | 10.0 | 398 | 0.004 |
| Anterior thalamic radiation R | 20.6 | 17.3 | 9.3 | 263 | 0.004 |
| Corticospinal tract L | −21.3 | −21.9 | 43.7 | 108 | 0.009 |
| Inferior fronto-occipital fasciculus L | −30.7 | 9.0 | 0.3 | 563 | 0.007 |
| Inferior fronto-occipital fasciculus R | 28.0 | 27.7 | 3.7 | 455 | 0.004 |
| Inferior longitudinal fasciculus L | −42.3 | −27.3 | −8.3 | 161 | 0.010 |
| Superior longitudinal fasciculus L | −38.8 | −10.9 | 26.3 | 188 | 0.008 |
| Superior longitudinal fasciculus R | 37.8 | −7.6 | 29.4 | 69 | 0.008 |
| Uncinate fasciculus L | −28.2 | 11.0 | −8.0 | 77 | 0.007 |
| Uncinate fasciculus R | 30.3 | 9.1 | −9.5 | 51 | 0.005 |
| (c) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 0.5 | 29.4 | 7.2 | 649 | 0.010 |
| Body of corpus callosum | −13.4 | 8.3 | 29.1 | 204 | 0.012 |
| Anterior corona radiata R | 16.5 | 34.8 | 3.0 | 90 | 0.011 |
| Anterior corona radiata L | −19.3 | 30.9 | 15.2 | 393 | 0.010 |
| Superior corona radiata L | −18.1 | 4.0 | 35.3 | 78 | 0.012 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −21.9 | 26.6 | 7.9 | 75 | 0.011 |
| Center of Gravity (mm Coordinates) | |||||
|---|---|---|---|---|---|
| X | Y | Z | Cluster Size | P(FWE-corr) | |
| (a) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 1.4 | 27.8 | 8.5 | 1372 | 0.003 |
| Body of corpus callosum | 1.4 | 1.4 | 25.7 | 1454 | 0.005 |
| Splenium of corpus callosum | 4.5 | −41.4 | 18.9 | 734 | 0.006 |
| Anterior limb of internal capsule R | 20.2 | 9.1 | 10.4 | 354 | 0.005 |
| Anterior limb of internal capsule L | −19.0 | 9.1 | 9.9 | 227 | 0.008 |
| Posterior limb of internal capsule R | 23.5 | −13.6 | 9.5 | 338 | 0.006 |
| Posterior limb of internal capsule L | −22.1 | −12.5 | 9.7 | 181 | 0.008 |
| Retrolenticular part of internal capsule R | 30.9 | −31.0 | 10.5 | 181 | 0.007 |
| Retrolenticular part of internal capsule L | −30.8 | −28.0 | 5.9 | 310 | 0.006 |
| Anterior corona radiata R | 23.3 | 25.8 | 10.1 | 906 | 0.005 |
| Anterior corona radiata L | −22.0 | 23.4 | 14.9 | 563 | 0.006 |
| Superior corona radiata R | 24.3 | −7.7 | 31.8 | 860 | 0.004 |
| Superior corona radiata L | −24.3 | −4.3 | 30.2 | 680 | 0.005 |
| Posterior corona radiata R | 24.9 | −37.7 | 28.3 | 316 | 0.006 |
| Posterior corona radiata L | −26.2 | −38.5 | 25.6 | 224 | 0.006 |
| Posterior thalamic radiation R | 33.0 | −50.0 | 13.9 | 189 | 0.008 |
| External capsule R | 29.2 | 0.7 | 3.7 | 199 | 0.007 |
| External capsule L | −31.7 | −8.9 | 4.7 | 415 | 0.006 |
| Superior fronto-occipital fasciculus R | 22.2 | 5.7 | 21.0 | 68 | 0.005 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −20.8 | 16.6 | 10.7 | 316 | 0.007 |
| Anterior thalamic radiation R | 20.2 | 14.2 | 9.3 | 248 | 0.005 |
| Corticospinal tract L | −23.3 | −21.9 | 31.3 | 298 | 0.006 |
| Corticospinal tract R | 23.8 | −21.4 | 28.0 | 474 | 0.005 |
| Inferior fronto-occipital fasciculus L | −31.0 | 10.0 | 1.8 | 370 | 0.006 |
| Inferior fronto-occipital fasciculus R | 27.8 | 30.8 | 5.0 | 365 | 0.005 |
| Inferior longitudinal fasciculus L | −42.6 | −21.4 | −9.2 | 73 | 0.007 |
| Superior longitudinal fasciculus L | −37.6 | −41.6 | 28.3 | 147 | 0.007 |
| Superior longitudinal fasciculus R | 36.8 | −23.5 | 31.8 | 476 | 0.006 |
| (b) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 1.0 | 27.8 | 8.6 | 1440 | 0.002 |
| Body of corpus callosum | −0.2 | 5.6 | 26.6 | 1332 | 0.004 |
| Splenium of corpus callosum | 13.7 | −41.6 | 20.4 | 283 | 0.012 |
| Anterior limb of internal capsule R | 20.3 | 9.8 | 9.9 | 328 | 0.005 |
| Anterior limb of internal capsule L | −18.4 | 8.8 | 9.2 | 312 | 0.005 |
| Posterior limb of internal capsule R | 21.1 | −5.5 | 10.9 | 56 | 0.007 |
| Retrolenticular part of internal capsule L | −32.3 | −28.8 | 4.8 | 188 | 0.010 |
| Anterior corona radiata R | 22.1 | 26.7 | 11.1 | 1155 | 0.004 |
| Anterior corona radiata L | −20.6 | 27.7 | 10.7 | 1012 | 0.004 |
| Superior corona radiata R | 23.5 | −0.8 | 31.9 | 607 | 0.005 |
| Superior corona radiata L | −22.5 | −2.3 | 31.7 | 513 | 0.005 |
| Posterior corona radiata R | 22.2 | −41.0 | 32.0 | 120 | 0.012 |
| Sagittal stratum L | −40.0 | −30.5 | −9.1 | 124 | 0.010 |
| External capsule R | 29.7 | 9.1 | −1.6 | 314 | 0.005 |
| External capsule L | −30.3 | −1.3 | 0.0 | 574 | 0.008 |
| Superior fronto-occipital fasciculus R | 22.2 | 5.6 | 21.2 | 64 | 0.004 |
| Superior fronto-occipital fasciculus L | −21.1 | 5.1 | 20.1 | 54 | 0.005 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −20.1 | 17.0 | 10.0 | 398 | 0.004 |
| Anterior thalamic radiation R | 20.6 | 17.3 | 9.3 | 263 | 0.004 |
| Corticospinal tract L | −21.3 | −21.9 | 43.7 | 108 | 0.009 |
| Inferior fronto-occipital fasciculus L | −30.7 | 9.0 | 0.3 | 563 | 0.007 |
| Inferior fronto-occipital fasciculus R | 28.0 | 27.7 | 3.7 | 455 | 0.004 |
| Inferior longitudinal fasciculus L | −42.3 | −27.3 | −8.3 | 161 | 0.010 |
| Superior longitudinal fasciculus L | −38.8 | −10.9 | 26.3 | 188 | 0.008 |
| Superior longitudinal fasciculus R | 37.8 | −7.6 | 29.4 | 69 | 0.008 |
| Uncinate fasciculus L | −28.2 | 11.0 | −8.0 | 77 | 0.007 |
| Uncinate fasciculus R | 30.3 | 9.1 | −9.5 | 51 | 0.005 |
| (c) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 0.5 | 29.4 | 7.2 | 649 | 0.010 |
| Body of corpus callosum | −13.4 | 8.3 | 29.1 | 204 | 0.012 |
| Anterior corona radiata R | 16.5 | 34.8 | 3.0 | 90 | 0.011 |
| Anterior corona radiata L | −19.3 | 30.9 | 15.2 | 393 | 0.010 |
| Superior corona radiata L | −18.1 | 4.0 | 35.3 | 78 | 0.012 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −21.9 | 26.6 | 7.9 | 75 | 0.011 |
Location of Significant Linear Relationship Between NES total and (a) axial diffusivity, (b) mean diffusivity, (c) radial diffusivity in patients with schizophrenia
| Center of Gravity (mm Coordinates) | |||||
|---|---|---|---|---|---|
| X | Y | Z | Cluster Size | P(FWE-corr) | |
| (a) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 1.4 | 27.8 | 8.5 | 1372 | 0.003 |
| Body of corpus callosum | 1.4 | 1.4 | 25.7 | 1454 | 0.005 |
| Splenium of corpus callosum | 4.5 | −41.4 | 18.9 | 734 | 0.006 |
| Anterior limb of internal capsule R | 20.2 | 9.1 | 10.4 | 354 | 0.005 |
| Anterior limb of internal capsule L | −19.0 | 9.1 | 9.9 | 227 | 0.008 |
| Posterior limb of internal capsule R | 23.5 | −13.6 | 9.5 | 338 | 0.006 |
| Posterior limb of internal capsule L | −22.1 | −12.5 | 9.7 | 181 | 0.008 |
| Retrolenticular part of internal capsule R | 30.9 | −31.0 | 10.5 | 181 | 0.007 |
| Retrolenticular part of internal capsule L | −30.8 | −28.0 | 5.9 | 310 | 0.006 |
| Anterior corona radiata R | 23.3 | 25.8 | 10.1 | 906 | 0.005 |
| Anterior corona radiata L | −22.0 | 23.4 | 14.9 | 563 | 0.006 |
| Superior corona radiata R | 24.3 | −7.7 | 31.8 | 860 | 0.004 |
| Superior corona radiata L | −24.3 | −4.3 | 30.2 | 680 | 0.005 |
| Posterior corona radiata R | 24.9 | −37.7 | 28.3 | 316 | 0.006 |
| Posterior corona radiata L | −26.2 | −38.5 | 25.6 | 224 | 0.006 |
| Posterior thalamic radiation R | 33.0 | −50.0 | 13.9 | 189 | 0.008 |
| External capsule R | 29.2 | 0.7 | 3.7 | 199 | 0.007 |
| External capsule L | −31.7 | −8.9 | 4.7 | 415 | 0.006 |
| Superior fronto-occipital fasciculus R | 22.2 | 5.7 | 21.0 | 68 | 0.005 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −20.8 | 16.6 | 10.7 | 316 | 0.007 |
| Anterior thalamic radiation R | 20.2 | 14.2 | 9.3 | 248 | 0.005 |
| Corticospinal tract L | −23.3 | −21.9 | 31.3 | 298 | 0.006 |
| Corticospinal tract R | 23.8 | −21.4 | 28.0 | 474 | 0.005 |
| Inferior fronto-occipital fasciculus L | −31.0 | 10.0 | 1.8 | 370 | 0.006 |
| Inferior fronto-occipital fasciculus R | 27.8 | 30.8 | 5.0 | 365 | 0.005 |
| Inferior longitudinal fasciculus L | −42.6 | −21.4 | −9.2 | 73 | 0.007 |
| Superior longitudinal fasciculus L | −37.6 | −41.6 | 28.3 | 147 | 0.007 |
| Superior longitudinal fasciculus R | 36.8 | −23.5 | 31.8 | 476 | 0.006 |
| (b) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 1.0 | 27.8 | 8.6 | 1440 | 0.002 |
| Body of corpus callosum | −0.2 | 5.6 | 26.6 | 1332 | 0.004 |
| Splenium of corpus callosum | 13.7 | −41.6 | 20.4 | 283 | 0.012 |
| Anterior limb of internal capsule R | 20.3 | 9.8 | 9.9 | 328 | 0.005 |
| Anterior limb of internal capsule L | −18.4 | 8.8 | 9.2 | 312 | 0.005 |
| Posterior limb of internal capsule R | 21.1 | −5.5 | 10.9 | 56 | 0.007 |
| Retrolenticular part of internal capsule L | −32.3 | −28.8 | 4.8 | 188 | 0.010 |
| Anterior corona radiata R | 22.1 | 26.7 | 11.1 | 1155 | 0.004 |
| Anterior corona radiata L | −20.6 | 27.7 | 10.7 | 1012 | 0.004 |
| Superior corona radiata R | 23.5 | −0.8 | 31.9 | 607 | 0.005 |
| Superior corona radiata L | −22.5 | −2.3 | 31.7 | 513 | 0.005 |
| Posterior corona radiata R | 22.2 | −41.0 | 32.0 | 120 | 0.012 |
| Sagittal stratum L | −40.0 | −30.5 | −9.1 | 124 | 0.010 |
| External capsule R | 29.7 | 9.1 | −1.6 | 314 | 0.005 |
| External capsule L | −30.3 | −1.3 | 0.0 | 574 | 0.008 |
| Superior fronto-occipital fasciculus R | 22.2 | 5.6 | 21.2 | 64 | 0.004 |
| Superior fronto-occipital fasciculus L | −21.1 | 5.1 | 20.1 | 54 | 0.005 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −20.1 | 17.0 | 10.0 | 398 | 0.004 |
| Anterior thalamic radiation R | 20.6 | 17.3 | 9.3 | 263 | 0.004 |
| Corticospinal tract L | −21.3 | −21.9 | 43.7 | 108 | 0.009 |
| Inferior fronto-occipital fasciculus L | −30.7 | 9.0 | 0.3 | 563 | 0.007 |
| Inferior fronto-occipital fasciculus R | 28.0 | 27.7 | 3.7 | 455 | 0.004 |
| Inferior longitudinal fasciculus L | −42.3 | −27.3 | −8.3 | 161 | 0.010 |
| Superior longitudinal fasciculus L | −38.8 | −10.9 | 26.3 | 188 | 0.008 |
| Superior longitudinal fasciculus R | 37.8 | −7.6 | 29.4 | 69 | 0.008 |
| Uncinate fasciculus L | −28.2 | 11.0 | −8.0 | 77 | 0.007 |
| Uncinate fasciculus R | 30.3 | 9.1 | −9.5 | 51 | 0.005 |
| (c) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 0.5 | 29.4 | 7.2 | 649 | 0.010 |
| Body of corpus callosum | −13.4 | 8.3 | 29.1 | 204 | 0.012 |
| Anterior corona radiata R | 16.5 | 34.8 | 3.0 | 90 | 0.011 |
| Anterior corona radiata L | −19.3 | 30.9 | 15.2 | 393 | 0.010 |
| Superior corona radiata L | −18.1 | 4.0 | 35.3 | 78 | 0.012 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −21.9 | 26.6 | 7.9 | 75 | 0.011 |
| Center of Gravity (mm Coordinates) | |||||
|---|---|---|---|---|---|
| X | Y | Z | Cluster Size | P(FWE-corr) | |
| (a) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 1.4 | 27.8 | 8.5 | 1372 | 0.003 |
| Body of corpus callosum | 1.4 | 1.4 | 25.7 | 1454 | 0.005 |
| Splenium of corpus callosum | 4.5 | −41.4 | 18.9 | 734 | 0.006 |
| Anterior limb of internal capsule R | 20.2 | 9.1 | 10.4 | 354 | 0.005 |
| Anterior limb of internal capsule L | −19.0 | 9.1 | 9.9 | 227 | 0.008 |
| Posterior limb of internal capsule R | 23.5 | −13.6 | 9.5 | 338 | 0.006 |
| Posterior limb of internal capsule L | −22.1 | −12.5 | 9.7 | 181 | 0.008 |
| Retrolenticular part of internal capsule R | 30.9 | −31.0 | 10.5 | 181 | 0.007 |
| Retrolenticular part of internal capsule L | −30.8 | −28.0 | 5.9 | 310 | 0.006 |
| Anterior corona radiata R | 23.3 | 25.8 | 10.1 | 906 | 0.005 |
| Anterior corona radiata L | −22.0 | 23.4 | 14.9 | 563 | 0.006 |
| Superior corona radiata R | 24.3 | −7.7 | 31.8 | 860 | 0.004 |
| Superior corona radiata L | −24.3 | −4.3 | 30.2 | 680 | 0.005 |
| Posterior corona radiata R | 24.9 | −37.7 | 28.3 | 316 | 0.006 |
| Posterior corona radiata L | −26.2 | −38.5 | 25.6 | 224 | 0.006 |
| Posterior thalamic radiation R | 33.0 | −50.0 | 13.9 | 189 | 0.008 |
| External capsule R | 29.2 | 0.7 | 3.7 | 199 | 0.007 |
| External capsule L | −31.7 | −8.9 | 4.7 | 415 | 0.006 |
| Superior fronto-occipital fasciculus R | 22.2 | 5.7 | 21.0 | 68 | 0.005 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −20.8 | 16.6 | 10.7 | 316 | 0.007 |
| Anterior thalamic radiation R | 20.2 | 14.2 | 9.3 | 248 | 0.005 |
| Corticospinal tract L | −23.3 | −21.9 | 31.3 | 298 | 0.006 |
| Corticospinal tract R | 23.8 | −21.4 | 28.0 | 474 | 0.005 |
| Inferior fronto-occipital fasciculus L | −31.0 | 10.0 | 1.8 | 370 | 0.006 |
| Inferior fronto-occipital fasciculus R | 27.8 | 30.8 | 5.0 | 365 | 0.005 |
| Inferior longitudinal fasciculus L | −42.6 | −21.4 | −9.2 | 73 | 0.007 |
| Superior longitudinal fasciculus L | −37.6 | −41.6 | 28.3 | 147 | 0.007 |
| Superior longitudinal fasciculus R | 36.8 | −23.5 | 31.8 | 476 | 0.006 |
| (b) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 1.0 | 27.8 | 8.6 | 1440 | 0.002 |
| Body of corpus callosum | −0.2 | 5.6 | 26.6 | 1332 | 0.004 |
| Splenium of corpus callosum | 13.7 | −41.6 | 20.4 | 283 | 0.012 |
| Anterior limb of internal capsule R | 20.3 | 9.8 | 9.9 | 328 | 0.005 |
| Anterior limb of internal capsule L | −18.4 | 8.8 | 9.2 | 312 | 0.005 |
| Posterior limb of internal capsule R | 21.1 | −5.5 | 10.9 | 56 | 0.007 |
| Retrolenticular part of internal capsule L | −32.3 | −28.8 | 4.8 | 188 | 0.010 |
| Anterior corona radiata R | 22.1 | 26.7 | 11.1 | 1155 | 0.004 |
| Anterior corona radiata L | −20.6 | 27.7 | 10.7 | 1012 | 0.004 |
| Superior corona radiata R | 23.5 | −0.8 | 31.9 | 607 | 0.005 |
| Superior corona radiata L | −22.5 | −2.3 | 31.7 | 513 | 0.005 |
| Posterior corona radiata R | 22.2 | −41.0 | 32.0 | 120 | 0.012 |
| Sagittal stratum L | −40.0 | −30.5 | −9.1 | 124 | 0.010 |
| External capsule R | 29.7 | 9.1 | −1.6 | 314 | 0.005 |
| External capsule L | −30.3 | −1.3 | 0.0 | 574 | 0.008 |
| Superior fronto-occipital fasciculus R | 22.2 | 5.6 | 21.2 | 64 | 0.004 |
| Superior fronto-occipital fasciculus L | −21.1 | 5.1 | 20.1 | 54 | 0.005 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −20.1 | 17.0 | 10.0 | 398 | 0.004 |
| Anterior thalamic radiation R | 20.6 | 17.3 | 9.3 | 263 | 0.004 |
| Corticospinal tract L | −21.3 | −21.9 | 43.7 | 108 | 0.009 |
| Inferior fronto-occipital fasciculus L | −30.7 | 9.0 | 0.3 | 563 | 0.007 |
| Inferior fronto-occipital fasciculus R | 28.0 | 27.7 | 3.7 | 455 | 0.004 |
| Inferior longitudinal fasciculus L | −42.3 | −27.3 | −8.3 | 161 | 0.010 |
| Superior longitudinal fasciculus L | −38.8 | −10.9 | 26.3 | 188 | 0.008 |
| Superior longitudinal fasciculus R | 37.8 | −7.6 | 29.4 | 69 | 0.008 |
| Uncinate fasciculus L | −28.2 | 11.0 | −8.0 | 77 | 0.007 |
| Uncinate fasciculus R | 30.3 | 9.1 | −9.5 | 51 | 0.005 |
| (c) | |||||
| JHU WM labels atlas | |||||
| Genu of corpus callosum | 0.5 | 29.4 | 7.2 | 649 | 0.010 |
| Body of corpus callosum | −13.4 | 8.3 | 29.1 | 204 | 0.012 |
| Anterior corona radiata R | 16.5 | 34.8 | 3.0 | 90 | 0.011 |
| Anterior corona radiata L | −19.3 | 30.9 | 15.2 | 393 | 0.010 |
| Superior corona radiata L | −18.1 | 4.0 | 35.3 | 78 | 0.012 |
| JHU WM tractography atlas | |||||
| Anterior thalamic radiation L | −21.9 | 26.6 | 7.9 | 75 | 0.011 |
The linear associations of the four WM parameters and the NES subscales were largely consistent with the results of the NES total score (see supplementary material tables 6–14). However, none of these associations would survive stringent correction for multiple comparisons.
Correlations of Motor Fiber Tracts With Neurological Soft Signs
The exploratory partial correlations (corrected for age and CPZ) between the SLF or the CST and NES total scores detected no associations. However, higher FA of the right aslant correlated with increased scores on the NES subscales motor coordination and sequence of complex motor tasks (P < 0.05) (see table S15 in the supplementary material and figure 2).
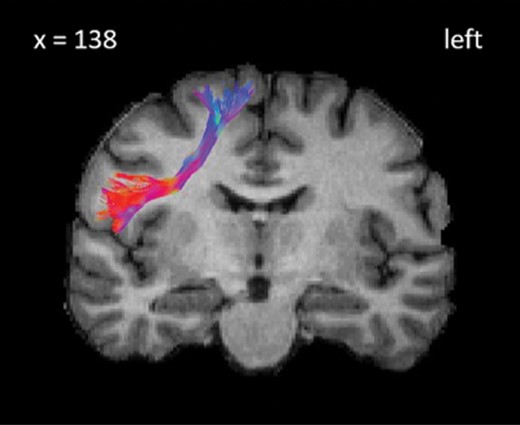
The image shows the reconstruction of the right aslant tract for a patient with schizophrenia.
Discussion
The aim of this study was to test whether the severity of Neurological Soft Signs was associated with white matter alterations in patients with schizophrenia. Indeed, NSS were linked to white matter changes of important motor pathways. While the total score of the NES scale was not associated with FA values, it was related to increases of white matter diffusivity, i.e. RD, MD, and AD. Furthermore, in our exploratory analysis we found a relationship between FA of the right aslant connecting the supplementary motor area (SMA) with the dorsolateral prefrontal cortex and the NES subscales motor coordination and sequence of complex motor tasks. Despite diverse results of NSS with each WM measure, we confirmed our hypothesis of an association between NES and WM changes in important motor pathways (e.g. corticospinal tract, corpus callosum, internal capsule, superior longitudinal fascicle) in patients with schizophrenia.
NSS were related to AD and MD values in overlapping white matter regions across the brain including important motor fiber tracts, such as corpus callosum, internal capsule, thalamic radiation, CST and SLF. In addition, significant associations of NSS with RD values were limited to the corpus callosum, corona radiata, and anterior thalamic radiations. All associations were positive, indicating that patients with severe NSS have higher AD, MD, and RD values of multiple WM regions suggestive of increased diffusivity. In our study, we found very few associations between NSS and WM alterations in the parietal lobe with MD and none with RD. This scarcity of association in the parietal lobe is somewhat unexpected, given the multiple reports of grey matter morphology changes linked to NSS in the somatosensory cortex.19,25
The main result of the study reveals an association of NSS with white matter alterations in the motor system in patients with schizophrenia. The WM areas linked to NSS include multiple fiber tracts that are important for motor function. The CST runs from the precentral motor area to the caudal brain stem69,70 and is a major spinal pathway for voluntary motor control.71 The internal capsule includes motor corticospinal fibers.69,72 This tract is crucial for perceptual and motor functions.73 Thalamocortical radiations connect the thalamus with different areas of the cerebral cortex and are critical for motor and sensory information processing.74 The fibers of the SLF run from the side of the putamen into all four lobes69 and serve the control of higher order motor behavior.75 The corpus callosum integrates information of both hemispheres and is essential for the processing of cognitive, sensory and motor information.76 In our exploratory analyses, we further found an association between the aslant tract and NSS. This fiber tract has been associated with motor actions and connects the SMA and pre-SMA with the posterior inferior frontal gyrus.77
Our results are in line with other neuroimaging studies reporting brain correlates of NSS in patients with schizophrenia.15,78 However, only a few studies investigated WM changes related to NSS. Two voxel-based morphometry studies reported associations between NSS severity and the volume or density of WM in schizophrenia.13,20 Likewise, a TBSS study in subjects at risk for psychosis found NSS to predict FA decrease in the superior cerebellar peduncle within one year.39 Finally, in line with our study, increased NSS were associated with lower FA, higher AD and RD values in the corpus callosum in stroke patients.79
Various other motor signs in schizophrenia are associated with WM changes. For instance, altered motor pathways have been associated with psychomotor slowing.80–82 Similarly, tardive dyskinesia, catatonia, and the motor dimension of the DSM-5 have been related to WM changes.83–86 Collectively, these WM studies corroborate findings from multiple other MRI methods in demonstrating a link between aberrant motor behavior and alterations in the cerebral motor system in psychosis.15,87,88
The neuropathology of schizophrenia includes altered myelination and dysfunction of oligodendrocytes.89 DTI studies confirmed white matter changes in schizophrenia.29,32 However, the interpretation of scalar measures remains difficult. The tensor is described by its eigenvalues, whereby the largest eigenvalue (AD) represents the main fiber orientation (water diffusion along the axons), and RD describes the water diffusion perpendicular to the fiber bundle, whereas FA describes the relationship between AD and RD,90 and MD describes the averaged magnitude of diffusion.91
Our findings are consistent with a neurodevelopmental model of schizophrenia and NSS.3,41,45 Motor pathways start to develop prenatally and maturation continues well into adulthood.35,36,92 Furthermore, studies linked neurodevelopmental delays to altered white matter maturation in the motor tracts of adolescents born preterm, e.g. increased MD and decreased FA in corpus callosum and CST.93 Likewise, in our study patients with schizophrenia had lower FA and increased MD and RD in white matter motor pathways compared to controls, which is in line with multiple studies in psychosis.29,30,32,94 These structural alterations are likely to be associated with subtle motor abnormalities, such as NSS.95 In fact, during childhood the acquisition of motor skills is linked to the maturation of major motor fiber tracts such as CST or corpus callosum.37,38 Children with lower motor performance had increased RD and MD, suggesting less efficient myelination or packing of fibers.37 Thus, both NSS and white matter abnormalities may indicate neurodevelopmental delay in schizophrenia.
Besides their potential in predicting the risk for or early course of psychosis, NSS also hold promise in identifying subjects with particularly poor functioning who require intense treatment effort.3,45,96,97 Antipsychotic treatment may ameliorate NSS in a group of patients who also seem to have a beneficial outcome, while patients with stable NSS tend to have poor long-term outcomes.98–101 Further deterioration of NSS was reported in older patients with schizophrenia.102 Given the heterogeneity of the course of NSS, we may speculate that white matter abnormalities along with morphometric grey matter alterations in motor regions constitute a marker of delayed or inefficient neuromaturation associated with NSS severity. The temporal dynamics of WM alterations, however, suggest that WM alterations fall short of explaining the entire presentation of NSS. Instead, we may consider these structural alterations to compromise connectivity and information flow in the motor circuitry,45 which is counter-balanced by effective functional connectivity before and after psychotic episodes. Still, during psychotic episodes, we expect a number of neurochemical alterations that may also compromise functional connectivity and thus drive faulty signaling within the motor circuitry,25,87,97 giving rise to more severe NSS. This combined detrimental effect of grey and white matter abnormalities and functional connectivity alterations in the motor circuitry would be able to account for the state and trait features of NSS.100
Some limitations of this study require discussion. Several variables may have an effect on WM integrity. For example, age has been related to WM changes103–105 and some white matter fiber tracts show accelerated aging effects in schizophrenia.28 In addition, severity of psychosis was related to reduced local white matter volume.106 Further, the effect of antipsychotic medication on myelination and white matter indices in psychosis is subject of an ongoing debate with conflicting findings.107,108 In addition, motor side effects of antipsychotic treatment may be misinterpreted as NSS.109 However, studies including medication-naïve patients demonstrate that NSS occur prior to antipsychotic treatment.2,3,109 Thus, we included age, antipsychotic medication, symptom severity and motion as covariates of no interest in our analyses. Another limitation is the conceptual overlap between multiple motor phenomena in schizophrenia.45,110 Other motor pathologies such as Parkinsonism, dyskinesia or catatonia may inflate NES ratings (see table S2 in the supplement), but limiting the sample to subjects without motor abnormalities other than NES would result in a very small sample size. Further, TBSS and tractography have specific limitations, and other methods, e.g. large scale network analysis of the connectome might reveal additional information on the association between NSS and WM. Finally, as NSS and WM might change over time, our cross-sectional study may fail to be valid across the entire life span of schizophrenia patients.
Conclusion
The main finding of our study indicates an association of Neurological Soft Signs in patients with schizophrenia and increased diffusivity in the CST, corpus callosum, and SLF. These findings in major motor white matter pathways may reflect the nature of NSS at the interface of basic and higher-order motor control. Structural and functional brain alterations may collectively explain the heterogeneous trajectory of NSS in psychosis.
Funding
This study received funding from the Bangerter-Rhyner Foundation (to Sebastian Walther), and the Swiss National Science Foundation (SNF grant 152619 to Sebastian Walther, Andrea Federspiel, and Stephan Bohlhalter).
Acknowledgments
We thank Isabel Reber for helping with the reconstruction of the fiber tracts. The authors have declared that there are no conflicts of interest in relation to the subject of this study.

{kind=link}
{kind=link}