




Abstract
The aim of this study was to explore barriers and facilitators in the implementation of a health course for adults with mild or moderate intellectual disabilities. An inductive qualitative design was used. Data were collected from a health course conducted in 16 study groups with 83 participants in Stockholm, Sweden by unstructured observations in course sessions, a group discussion with course leaders and evaluation notes from the course leaders. The data were analysed by qualitative content analysis. Four categories were identified: (i) ‘individual characteristics’, implying various needs, (ii) ‘pedagogical strategies’ used to meet those needs, (iii) ‘interaction within the course’, dealing with active and less active participation and (iv) ‘structures’, including learning climate and organizing. The overarching theme ‘creating an individualized supportive context’ describes the challenge of educating people with intellectual disabilities towards an empowered and well informed decision making regarding their own health. Therefore, there is a need for support not only within the course but also from the social and physical environment as well.
Introduction
People with intellectual disabilities are at high risk of several behavioural risk factors for ill-health, such as poor dietary habits [1, 2], low physical activity [3–5] and weight disturbances [4, 6, 7], increasing the risk for chronic diseases [8, 9]. The higher disease burden among people with disabilities can partly be explained by barriers in accessing services, such as health, education, employment and information [10]. Research shows that people with intellectual disabilities do not participate in society on equal terms, as their specific difficulties are not adequately taken into consideration [11].
To be able to participate in society people with intellectual disabilities are in need of support. In Sweden, the Act Concerning Support and Services for Persons with Certain Functional Impairments regulates rights for individuals with intellectual disabilities and, according to this act, all support must be based on self-determination and integrity [12]. Caregivers trying to support healthy behaviours without encroaching on autonomy often face ethical dilemmas [13] which causes uncertainty in how to give support in the most appropriate way [14].Therefore, it is important to foster empowerment of people with intellectual disabilities to make their own healthy choices.
According to Cattaneo and Chapman [15] empowerment can be defined as an iterative process in which the individual has to develop self-efficacy, knowledge and competence to be able to set personally meaningful goals. By increasing empowerment the individuals’ abilities to take own responsibility in health decisions is enhanced. To make these decisions the individual needs relevant expertise, which is the core of the concept health literacy [16].
Health literacy refers to the knowledge and competencies of accessing, understanding, appraising and applying health-related information [17]. Low health literacy is associated with poorer health outcomes and poorer use of health care services [18]. Health literacy is essential to make informed decisions but cannot be used as motivation for action in itself, which distinguishes the concept from the concept of empowerment [16]. It is therefore important to increase both health literacy, which enables people to make informed choices, as well as to support the empowerment process, to increase the possibilities for people to gain control over the choices they make.
Health education might be used to improve health literacy [19] and has shown to be an effective way to improve health behaviours and as a consequence also healthy weight [20–22] as well as health knowledge and coping strategies [23] among people with intellectual disabilities. A variety of health education strategies might be appropriate since the learning styles vary [24]. Promising approaches include concrete instructions [25], practicing skills the students are about to learn [26], pictoral instructions and interactive activities [27]. However, most intervention studies describe the process of education very briefly, which means that knowledge about the significance of different approaches in relation to empowerment and learning is limited.
The aim of this study was to explore barriers and facilitators in the implementation of a health course for adults with mild or moderate intellectual disabilities.
Methods
The health course was part of a more extensive health intervention that was carried out in community residences in Stockholm, Sweden [28].
Description of the health course
The health course was designed for adults with mild or moderate intellectual disabilities. It was developed by a Swedish national educational association (Studieförbundet Vuxenskolan) during a 2-year project, in which four study groups participated [29]. A written manual based on previous practise and experiences was developed and used for the courses within the present study [29].
The aim of the course was to improve health literacy and health-related behaviours in a positive way [29]. The content covered five areas: diet, physical activity, mental health, relaxation and culture/aesthetics, such as painting and other creative activities. The course included 10 sessions, 90 min each, held once a week. Each course was led by a course leader from the national educational association, who received 1 day of education focusing on the content of the manual. The education was organized by the educational association.
The manual included 10 suggested themes, one for each of the 10 sessions, such as ‘a tasty and healthy breakfast’ and ‘foreign countries’, when the participants could try out healthy foods and activities from other cultures. A list of 25 alternative themes was provided in case one particular theme did not fit. According to the manual each session should begin with a small group discussion, giving every participant the possibility to share their thoughts. All sessions included the preparation and tasting of a healthy meal/snack and some kind of physical activity or exercise. Each session was to finish by regrouping the participants for a brief discussion and to present the week’s assignment. Examples of assignment could be to try out healthy snacks or to perform a physical activity at home.
The manual included different tutorial materials to choose from as well as an individual health plan which was intended for caregivers or relatives who wanted to support the individual. The participants were given a binder for papers they received during the course, such as recipes and exercise programs. At the end of the course they received a diploma as a motivational reward, the ‘Driver’s license of health’.
Setting and participants
The course was conducted for the residents in 16 community residences, by eight course leaders (Table I). In some cases, when it was asked for and there was room for it, residents in neighbouring residences were invited as well. The course was scheduled in collaboration with caregivers and conducted within the residences when possible. In a few cases, other localities were used. The participant’s relatives and trustees were informed by a letter, but not involved in any other way.
Description of the 16 studied health courses and sources for data collection
| Course | Participants, men/women n = 83 | Course leadersan = 8 | Evaluation notes from course leaders n = 114 | Observations n = 6 | Course leaders in group discussionan = 5 |
|---|---|---|---|---|---|
| 1 | 3/3 | A + B | 10 | — | X |
| 2 | 2/4 | C | 0 | — | X |
| 3 | 0/2 | D | 10 | X | — |
| 4 | 4/2 | E | 0 | — | X |
| 5 | 2/3 | F | 10 | X | X |
| 6 | 2/3 | G | 2 | — | — |
| 7 | 1/5 | G | 4 | X | — |
| 8 | 1/7 | G | 4 | X | — |
| 9 | 3/2 | H | 9 | — | — |
| 10 | 2/2 | H | 6 | — | — |
| 11 | 2/1 | H | 10 | — | — |
| 12 | 3/1 | F | 10 | X | X |
| 13 | 3/4 | H | 10 | — | — |
| 14 | 4/2 | A + B | 9 | — | X |
| 15 | 3/2 | F | 10 | — | X |
| 16 | 2/3 | F | 10 | X | X |
| Course | Participants, men/women n = 83 | Course leadersan = 8 | Evaluation notes from course leaders n = 114 | Observations n = 6 | Course leaders in group discussionan = 5 |
|---|---|---|---|---|---|
| 1 | 3/3 | A + B | 10 | — | X |
| 2 | 2/4 | C | 0 | — | X |
| 3 | 0/2 | D | 10 | X | — |
| 4 | 4/2 | E | 0 | — | X |
| 5 | 2/3 | F | 10 | X | X |
| 6 | 2/3 | G | 2 | — | — |
| 7 | 1/5 | G | 4 | X | — |
| 8 | 1/7 | G | 4 | X | — |
| 9 | 3/2 | H | 9 | — | — |
| 10 | 2/2 | H | 6 | — | — |
| 11 | 2/1 | H | 10 | — | — |
| 12 | 3/1 | F | 10 | X | X |
| 13 | 3/4 | H | 10 | — | — |
| 14 | 4/2 | A + B | 9 | — | X |
| 15 | 3/2 | F | 10 | — | X |
| 16 | 2/3 | F | 10 | X | X |
aAs there was only one man as course leader, men and women are not accounted for due to confidentiality reasons.
Description of the 16 studied health courses and sources for data collection
| Course | Participants, men/women n = 83 | Course leadersan = 8 | Evaluation notes from course leaders n = 114 | Observations n = 6 | Course leaders in group discussionan = 5 |
|---|---|---|---|---|---|
| 1 | 3/3 | A + B | 10 | — | X |
| 2 | 2/4 | C | 0 | — | X |
| 3 | 0/2 | D | 10 | X | — |
| 4 | 4/2 | E | 0 | — | X |
| 5 | 2/3 | F | 10 | X | X |
| 6 | 2/3 | G | 2 | — | — |
| 7 | 1/5 | G | 4 | X | — |
| 8 | 1/7 | G | 4 | X | — |
| 9 | 3/2 | H | 9 | — | — |
| 10 | 2/2 | H | 6 | — | — |
| 11 | 2/1 | H | 10 | — | — |
| 12 | 3/1 | F | 10 | X | X |
| 13 | 3/4 | H | 10 | — | — |
| 14 | 4/2 | A + B | 9 | — | X |
| 15 | 3/2 | F | 10 | — | X |
| 16 | 2/3 | F | 10 | X | X |
| Course | Participants, men/women n = 83 | Course leadersan = 8 | Evaluation notes from course leaders n = 114 | Observations n = 6 | Course leaders in group discussionan = 5 |
|---|---|---|---|---|---|
| 1 | 3/3 | A + B | 10 | — | X |
| 2 | 2/4 | C | 0 | — | X |
| 3 | 0/2 | D | 10 | X | — |
| 4 | 4/2 | E | 0 | — | X |
| 5 | 2/3 | F | 10 | X | X |
| 6 | 2/3 | G | 2 | — | — |
| 7 | 1/5 | G | 4 | X | — |
| 8 | 1/7 | G | 4 | X | — |
| 9 | 3/2 | H | 9 | — | — |
| 10 | 2/2 | H | 6 | — | — |
| 11 | 2/1 | H | 10 | — | — |
| 12 | 3/1 | F | 10 | X | X |
| 13 | 3/4 | H | 10 | — | — |
| 14 | 4/2 | A + B | 9 | — | X |
| 15 | 3/2 | F | 10 | — | X |
| 16 | 2/3 | F | 10 | X | X |
aAs there was only one man as course leader, men and women are not accounted for due to confidentiality reasons.
The community residences participated in a larger health intervention, targeting residences for adults with mild or moderate intellectual disabilities [28]. All residences that had conducted or were conducting the course at the time of the study were included. Participation in the health course was voluntary. In total, 83 individuals (Table I) participated in the courses, among which 87% took part in at least 5 of the 10 sessions. Common reasons for not participating were not feeling well or prioritizing other activities. The participants were aged 20–63 years and 62% were women. All the participants had mild or moderate intellectual disabilities and some of them had additional physical disabilities, such as limited mobility, sensory loss or speech impediments.
The national educational association provided the course leaders, and made the choice of leader for each study group, according to geographical location and time schedule needs. Of the eight course leaders, seven were women and their age ranged from ∼30 to 60 years. Education and experience among the course leaders varied. They all had some experience from education or health care, for example, as study circle leaders, former teachers or caregivers. Some of them had experience of people with intellectual disabilities and no one had met any of the participants before. Two course leaders led two courses together, according to their own choice.
Data collection
An inductive qualitative design was used, since qualitative methods permit the researcher to study selected issues in depth and detail [30]. To obtain different perspectives, data were collected through three sources: (i) evaluation notes from course leaders, (ii) observations during course sessions and (iii) a group discussion with course leaders (Table I). By using several sources for data collection, triangulation was achieved, which supports trustworthiness of the study [30]. Data were collected between September 2010 and March 2012.
Evaluation notes from course leaders
Evaluation notes from the course leaders were collected to monitor the development of the courses. Each course leader was asked to write short notes, following a template, after each session. The notes described what worked well, which barriers the course leaders had encountered and ‘other reflections’. In total, 114 notes were received from six of the eight course leaders, covering 14 of the 16 courses.
Observations during course sessions
Observation was chosen as method for data collection since it provides insight into interactions and captures context and process [31], which makes it a preferable method when exploring what is happening during a group activity. By using observations it is possible to see things that otherwise might escape conscious awareness, since situations hidden within everyday routines might be taken for granted [30].
Six sessions, in six different community residences, were chosen for observation. Since the courses started and ended at different points in time sessions were chosen by convenience sampling [30] in agreement with the course leaders. All observations were carried out in the community residences by the first author (H.B.) and lasted for 70–120 min. Short field notes were taken during the observation and were rewritten in more detail immediately after, since it was important to record field notes as closely in time as possible to when events were observed [31]. In addition to the actual observations, the observer included her own reflections and notes from informal conversations with the course leaders.
The observer played the role of ‘observer-as-participant’, who spends most of the time observing, with only a small proportion of time spent participating in normal group activity [32]. The observer mainly kept silent, but responded to questions and participated in some of the exercises, to make the group feel comfortable. The observations were unstructured—allowing the observer freedom to collect information that was unique to individual incidents—and overt, in the sense that participants were informed about the observation and the reason for it [33].
Group discussion with course leaders
To capture the attitudes and experiences among course leaders a group discussion was conducted, inspired by focus group discussion methodology [34]. In this study the course leaders had been working individually and it was assumed that a group discussion would enrich the data as they would be able to compare and discuss their experiences of barriers and facilitators in conducting the courses.
All eight course leaders were invited to a group discussion, and five participated. The three course leaders who did not participate indicated that the scheduled time did not fit. Some of the course leaders had already finished their courses when the discussion was held, while others had still ongoing courses. The date was chosen close to the courses in time, not allowing the course leaders to forget important issues. The discussion was held at the researcher’s workplace and lasted for 90 min. The first author (H.B.) acted as moderator for the discussion, and an assistant took notes. The participants were encouraged to talk to each other rather than addressing the researcher [34]. Questions were discussed in the group, concerning four predetermined topics: (i) the target group, (ii) the pedagogical situation, (iii) cooperation and support and (iv) practical issues. The group discussion was audiotaped and transcribed verbatim by the first author (H.B.).
Ethical considerations
Ethical considerations in observational studies regard the fact that situations might arise that are sensitive to the participants. Because of intellectual and cognitive limitations among the participants in this study, extra precautions were taken. All participants were informed that participation in this study was voluntary. The information was given in easy-to-read Swedish and caregivers who knew the participants well were assisting in understanding the information. They were promised confidentiality in the reports and gave their written consent to participation. Ethical permission was obtained from the Regional Ethical Review Board in Stockholm County Dnr. 2009/1332-31/5.
Analysis
The observations, group discussion and the evaluation notes were first analysed separately and then integrated to a coherent whole. The analysis was first performed by qualitative content analysis on a manifest level, according to the procedure described by Graneheim and Lundman [35]. The texts were divided into units of meaning, which were then condensed and labelled with codes. The codes were compared based on differences and similarities and sorted into categories and sub-categories. Each category and sub-category was illustrated with excerpts from the observations, the group discussion or the evaluation notes to show the connections to the original data. Ultimately an overarching theme, at a latent level, emerged from the contents of all the categories.
Analysis was performed by the first author (H.B.) and discussed continuously with the last author (U.W.). The theme, as well as categories and sub-categories, was defined by inter-subjective agreement between the authors to enhance trustworthiness of the study [35]. In cases of disagreement, the transcripts were carefully reread until consensus on the categorization was reached.
Results
The results identified an overarching theme at a latent level; creating an individualized supportive context, and four descriptive categories at a manifest level: (i) individual characteristics, (ii) pedagogical strategies, (iii) interaction within the course and (iv) structures. An overview of the results is given in Table II. Each category describes both barriers and facilitators in the implementation of the health course.
Barriers and facilitators in the implementation of the health course for individuals with intellectual disabilities
| Theme | Creating an individualized supportive context | |||
|---|---|---|---|---|
| Main categories | Individual characteristics | Pedagogical strategies | Interaction within the course | Structures |
| Sub-categories | Physical function | Trust and security | Participation | Planning and organizing |
| Cognitive function | Strategies for various senses | Communication | Physical environment | |
| Motivation | Support and adaptation | Staff involvement | Routines for collaboration | |
| Self-efficacy | Support for course leaders | |||
| Theme | Creating an individualized supportive context | |||
|---|---|---|---|---|
| Main categories | Individual characteristics | Pedagogical strategies | Interaction within the course | Structures |
| Sub-categories | Physical function | Trust and security | Participation | Planning and organizing |
| Cognitive function | Strategies for various senses | Communication | Physical environment | |
| Motivation | Support and adaptation | Staff involvement | Routines for collaboration | |
| Self-efficacy | Support for course leaders | |||
Barriers and facilitators in the implementation of the health course for individuals with intellectual disabilities
| Theme | Creating an individualized supportive context | |||
|---|---|---|---|---|
| Main categories | Individual characteristics | Pedagogical strategies | Interaction within the course | Structures |
| Sub-categories | Physical function | Trust and security | Participation | Planning and organizing |
| Cognitive function | Strategies for various senses | Communication | Physical environment | |
| Motivation | Support and adaptation | Staff involvement | Routines for collaboration | |
| Self-efficacy | Support for course leaders | |||
| Theme | Creating an individualized supportive context | |||
|---|---|---|---|---|
| Main categories | Individual characteristics | Pedagogical strategies | Interaction within the course | Structures |
| Sub-categories | Physical function | Trust and security | Participation | Planning and organizing |
| Cognitive function | Strategies for various senses | Communication | Physical environment | |
| Motivation | Support and adaptation | Staff involvement | Routines for collaboration | |
| Self-efficacy | Support for course leaders | |||
Creating an individualized supportive context
The overarching theme emerged out of the contents of the four categories. It describes the importance of an individualized supportive context when encouraging people with intellectual disabilities towards an empowered decision making regarding their own health. There is a need for support not only within the course but also from the social and physical environment as well. To extend the use of skills learned within the course to everyday life, it is important that the environment supports the use of those skills.
Individual characteristics
Individual characteristics varied among the participants, implying different needs in terms of the theoretical level of the education and the pedagogical strategies.
Physical function
Various functional limitations were represented, such as restricted mobility, difficulties with fine motor skills, sensory impairments, speech impediments and allergy and food hypersensitivity. These limitations affected the participants’ ability to take part in different activities. For example, restricted mobility hindered some outdoor activities, allergy forced some participants to decline trying out new foods and impaired vision or hearing sometimes complicated the perception of instructions.
The course leader asks the participants to stand on the floor to do Qi Gong. Participants 3 stands in front of the course leader, nearby, as she has difficulties seeing (Observation in course 5)
Cognitive function
The intellectual and cognitive levels of the participants varied. Cognitive abilities that were observed to affect the learning situation included communicative skills, memory, ability to concentrate and ability to understand instructions. Some participants were concentrated in the beginning of the session but their attention waned. In some situations there were participants who did not grasp what was expected, which sometimes resulted in feelings of insecurity. The course leaders were not always sure whether the participants understood or not.
Sometimes you think that the participants understand, and then you can see that sometimes they did, sometimes they didn’t. (Evaluation notes from course 3)
Motivation
Interest and motivation among the participants varied. Some residents chose not to take part at all, due to lack of interest or other priorities. Other participants chose not to take part in specific activities within the course. Feelings of enthusiasm and curiosity were also commonly observed, however. Some of the participants showed an interest in health issues and others enjoyed the social gathering. In some situations, rewards were motivating.
The course leader pulls the licenses from the bag and shows two laminated licenses with the participants’ photos. They receive them and examine them carefully. They look happy. (Observation in course 3)
Self-efficacy
In some of the situations when the participants did not want to take part in an activity, this seemed to be due to fear of the unknown. Unwillingness to participate was observed especially when new activities or foods were presented. Sometimes the participants chose not to take part, but in other situations initial doubts turned into a decision to give it a try.
When a participant dared to try out new activities, pride in performance was sometimes observed, as well as thoughts of transferring new knowledge into practice. For example, some participants asked where to find specific foods or music, for use in their own homes.Participant 3 first says that she doesn’t want orange in her smoothie, but then changes her mind. “I want to try the orange. I don’t give up.” (Observation in course 12)
Pedagogical strategies
The course leaders used different pedagogical strategies in their attempts to make the participants feel secure, and to meet the needs of participants with different cognitive levels and various learning preferences, thus providing individually adapted support.
Trust and security
The course leaders used repetition to create a feeling of security, such as indicating the beginning and the end of a course session by gathering the group and following specific routines. One course leader used a red fabric heart, which was passed around among the participants, to indicate whose turn it was to speak. Other ways to create trust and security included repeating what the group had done at the last session and giving clear information about what was going to happen at future sessions. Assignments and follow-up of assignments constituted a routine in some of the courses. According to the course leaders, deviations from the routines sometimes resulted in insecurity among the participants.
We changed to a different room because we were going to have two groups together. Then it happened again, that he wanted to go home. And that was because we had changed rooms that time. (Group discussion)
Strategies for various senses
All the observed course leaders informed about health issues by talking about them and one of them (G) told vivid stories, which she illustrated by using her own body. One course leader (F) based several discussions on issues that were brought up in the group interaction, while two others (D and G) frequently used books and pictures to discuss health topics. All the course leaders often used practical exercises, such as cooking, gymnastics, massage, relaxation and various creative activities. The participants were often encouraged to use their senses, for example, when experiencing nature or trying new foods.
The course leader says she has more varieties and dishes up almonds coated with orange. She sends them around so that anyone who wishes can try them, and asks everyone to smell, look and listen to how it sounds. (Observation in course 7)
Support and adaptation
The course leaders supported the participants by encouraging them to take part in different activities, giving feedback, assisting when needed and in some situations by using rewards. They made efforts to adapt the content of the course to the group as well as to the individuals within the group. In some of the groups, significant differences in intellectual and cognitive levels among the participants were observed. In some situations it became difficult for the course leaders to adapt the content to all participants; this sometimes resulted in activities being too advanced for some of the participants and too simple for others, as in the example below, when a bored participant wanted to choose another activity for herself:
The course leader tells everyone to paint fruits and reminds them of the fruits they have been talking about. (–-) Participant 5 asks if she can take a look in the book now. (Observation in course 7)
Interaction within the course
Interaction was observed more often between the course leaders and the participants than between the participants. In addition, the participants took a more or less active part in the detailed planning of the course content.
Participation
The observed course leaders mainly decided the content of each course session on the basis of the manual. They tried to involve the participants in planning parts of the content and encouraged them to share ideas. The extent to which the participants took active part in the planning varied. While some participants did only what they were told, others brought along their own materials, such as books or healthy snacks. It also happened that a participant invited the group to his or her home, as in this example:
All the participants did not take active part in the planning, however, and during the group discussion the course leaders expressed a wish to involve the participants to a greater extent.Together we had planned a feast and we were invited to one of the participants, where we set table for dinner and had a nice final day of the course. (Evaluation notes from course 16)
Communication
The communication patterns varied between the different observations (Fig. 1). In observations in courses 3, 7 and 8 (course leaders D and G) it was mainly directed one way, by the course leader posing questions, whereas in courses 5, 12 and 16 (course leader F) communication was to a larger extent initiated by the participants. The communication patterns were affected by the pedagogical strategies as well as by the composition of the groups. For example, interaction between the participants was difficult in course 3, since there were only two participants, and one was not very verbally communicative.
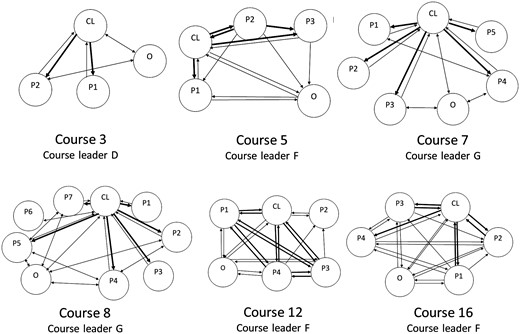
{kind=link}
Illustration of placing and communication patterns in the six observed health course sessions for individuals with intellectual disabilities. CL, course leader; P, participant; O, observer. The arrows indicate the direction and frequency of interaction.
The course constituted an arena for social interaction and fellowship, and the participants mostly showed a warm and permissive attitude towards each other, and assisted each other when needed. However, there were also situations when negative attitudes were observed, as in this example:
Participant 2 clearly shows that she intends to sit on the couch and not participate in any physical activity. “It is enough that I put on the music”, she says. The group does the first movement for a while, then changes to another involving stretching the arms toward the ceiling. “Participant 3, you do it too fast”, laughs Participant 2 from the couch. (Observation in course 5)
Staff involvement
The courses provided an opportunity for the inhabitants from one residence, and sometimes from neighbouring residences as well, to meet in a group activity. Most courses were carried out without the presence of caregivers, and there were only a few exceptions when caregivers participated due to the needs of the participants. According to the course leaders, a course without caregivers’ presence provided an opportunity for the participants to increase autonomy. The course leaders expressed that the caregivers were not well informed about the course. When they participated they sometimes interfered too much and when they did not participate they occasionally disturbed the sessions, by entering the room to do routine work.
The participants lie down on cushions on the floor and the course leader turns off the lights so that it becomes semi-dark in the room. “Now you may begin your journey to a large garden, where there are lots of flowers”. The course leader’s voice is calm and relaxed. “Now you are falling asleep.” It becomes silent in the room. Suddenly a caregiver comes in and says out loud, “Oh, it’s dark in here.” (Observation in course 8)
Structures
Structural factors affecting the course and the prerequisites for a good learning climate included planning and organizing, the physical environment, routines for collaboration with caregivers and other people within the social environment as well as support for the course leaders.
Planning and organizing
Before the start of each course, the course leaders visited the residences to inform about the course and to schedule it together with caregivers and potential participants. To find a time point when everyone could attend was not always easy, and most courses were scheduled for evenings or weekends. Most courses were conducted within the residence which, according to the course leaders, was appreciated by the participants.
Since all the inhabitants at each community residence were invited and sometimes those living at neighbouring residences as well, there were variations in size between the groups and variations in level of disability within the groups. In the group discussion, the course leaders expressed that having relatively homogenous groups in terms of intellectual abilities, comprising of ∼4–6 participants, would facilitate adaptation of the course content.
That level, okay then I know the level and I can plan the course around it. But if there are two or three different levels, then it might be a bit frustrating for a leader. Who should I consider? The one who knows a lot or who doesn’t. (Group discussion)
Physical environment
The sessions were held in a kitchen or living room at the residences, except for two themes that required outdoor activities. The environment was familiar to the participants, but in some cases the rooms used did not seem to be spacious enough.
The course leaders also expressed that it was important to have access to appropriate equipment, such as kitchen utensils and a sound system. Since the residences were in different locations, the possibilities for outdoor activities varied and a range of suitable areas nearby were used, such as small parks or walking paths. On some occasions the outdoor activities were cancelled due to bad weather, icy conditions or darkness.It’s pretty cramped in the kitchen, and two of the participants are standing partly in the hallway. (Observation in course 16)
Routines for collaboration
There were no routines for collaboration with caregivers and other significant people in the participant’s lives, except one initial meeting with caregivers. However, in the group discussion the course leaders expressed that well-functioning collaboration with caregivers was important.
In some residences the caregivers facilitated the course and supported the participants by reminding them about the course or following up on assignments between the sessions. The course leaders gave several examples of situations where the collaboration with caregivers did not work as well though. Some caregivers were difficult to get hold of and in many cases they did not provide support to the participants to accomplish the course. The individual health plan, which was included in the manual as an option for relatives or caregivers who wanted to support the participant, was not used by anyone. With relatives, trustees, day centres and residents’ organizations there was scarcely any collaboration.But when you look at the big picture and what this will lead to and what it will be like in the future, then it comes back to the caregivers. It’s about how to get them motivated. (Group discussion)
Support for course leaders
The course leaders emphasized that they needed relevant support to be able to conduct their task in a satisfactory way. Time management and economical compensation was important issues since they had to combine the courses with other work. They especially stressed that a lot of time was needed for preparations. Another issue raised was a wish for support from each other, by exchanging ideas and discuss experiences.
I think that we should meet more often, to exchange ideas. ‘How did you do? I did like this’ Then we can improve all the time. (Group discussion)
Discussion
The major results of this study imply that it is important to create an individualized supportive context when planning a health course for people with intellectual disabilities, to enable healthy behavioural changes within everyday life. This support should aim at fostering participation in society on equal terms and has to be present not only in the learning situation but also in the physical and social environment outside course sessions.
There was a wide variation in individual characteristics among the participants with regard to physical and cognitive abilities as well as motivation and self-efficacy. This variation was anticipated at a general level, but a more rigorous initial assessment of each participant could have facilitated adaptation of the course content to higher degree. The course leaders used different pedagogical strategies to meet the different needs and to achieve the course aim of improving health literacy and healthy behaviours. The task of health professionals in health communication is to enhance health literacy that enables people to make informed choices and to support them in developing empowerment to take control of their own situation [16].
The importance of matching strategies to the abilities of individuals with intellectual disabilities has previously been emphasized [26]. The course leaders mainly followed the course manual and tried to adapt the content not only to the abilities of the participants but also to different learning styles, by using pedagogic strategies to support kinaesthetic learners, visual learners and auditory learners. The use of different teaching methods is in accordance with previous research, since the learning styles of people with intellectual disabilities vary [24]. If the group was too heterogeneous it was challenging for the course leaders to adapt the course to all participants. For this reason, they wished the participants of future courses to have more similar levels of intellectual and cognitive ability. Not all the course leaders were used to work with people with intellectual disabilities or were trained educators which might have been a barrier to the employment of appropriate pedagogical strategies.
The interactional patterns during course sessions indicated dominance from the course leader. This has previously been identified in classroom situations as well as between caregivers and people with intellectual disabilities in regular conversations [36, 37]. Some of the dominance can be explained by the tutorial role of a course leader, but that does not exclude possibilities for interaction-based learning [36]. This was shown by course leader F, who based the educational strategies on the contributions of the participants, which resulted in livelier communication and interaction in these groups than in the other groups. In the smallest and largest groups, interactional difficulties were observed, which can probably be attributed to both group size and pedagogical strategies. However, ideal group size and similar levels of ability in a course must be weighed against the advantage of holding the course in a familiar social context with greater possibilities of support in daily routines.
According to Cattaneo and Chapman [15] goal setting is an important dimension of the empowerment process. The aim of the health course was to support the participants in improving their health literacy and health behaviour, but in most cases no individual goals had been set and thus no actions towards the goal could be taken. The individual health plan of the manual, which was intended for caregivers and relatives, was not used, which might have been due to the limited collaboration with caregivers and relatives. To increase empowerment, individual goal setting should also be included and evaluated [15].
The social context is regarded important to empowerment since it constrains or facilitates the efforts of the individual [15]. The participant’s caregivers, trustees and relatives are crucial elements in the social context. The importance of the caregivers’ involvement was emphasized in a review of weight loss interventions: people with intellectual disabilities often make lifestyle choices collaboratively with their caregivers [38]. Therefore, time needs to be spent not only to plan the contents of the course itself but also to plan how to include caregivers, relatives and other significant people within the context surrounding the course.
The caregivers were informed about the course and their role in relation to the course at various meetings. However, the residents and the course leaders did not take part in those meetings. More effective collaboration could possibly have been achieved by more frequent communication between the course leaders and the caregivers, enabling discussion about how to support the participants during and after the course period. The participant’s trustees and relatives, as well as day centre staff, could also have been involved to create a more individualized supportive context.
To develop and maintain new skills the participants need opportunities and support to practice those new skills. The difficulty of maintaining skills that are seldom needed or practiced was noted in a study regarding education of people with intellectual disabilities on safety skills [26]. Eating and physical activity are practiced daily. Nonetheless it is important that caregivers, trustees and relatives are well informed and motivated to support new skills, for example, by accompanying the residents to the store to buy healthy foods or by going along to different activities.
Efforts were made to find times when everyone could attend. Since many of the residents spend several hours daily in day centres another possibility could be to introduce a health course as a day centre activity instead of a leisure time activity. More women than men attended the course, which might imply that the content attracted women more than men. Since women with intellectual disabilities are at higher risk of ill-health than men, women are important to reach [3, 4, 6, 9].
Strengths and weaknesses
To our knowledge no previous studies have attempted to understand the barriers and facilitators within the process of health education for adults with intellectual disabilities in community residences. A strength of this study is therefore that it is among the first to empirically study challenges in the implementation of a health course for people with intellectual disabilities, conducted within their everyday environment.
Data were collected from three different sources. This triangulation of data supports the trustworthiness of the study, as do the illustrative excerpts and inter-subjective agreement in the process of analysis [30]. Focus group discussions or interviews with the participants could have enriched the data. By using observations attention was given to all participants though, also the ones that had difficulties to express themselves verbally. Data were collected from all eight course leaders, although only three were included in the observations. Since the study sample is small the results are not generalizable, but should be of interest and possible to transfer to similar contexts.
The observer/interviewer was slightly acquainted with the participants because they were included in a larger health intervention, in which the observer/interviewer was involved as a researcher. These insights of pre-understanding were judged to be positive and useful to attain a deeper understanding, but the potential for bias was always kept in mind during the interpretation of the data. The last author (U.W.) was neither involved in the intervention nor familiar with the participants. Analysis was, therefore, continuously discussed with her to prevent the pre-understanding from biasing the interpretation.
Conclusions
The health course offered good opportunities for the participants to increase health literacy in a group activity where they, without the presence of caregivers, got the possibility to practice autonomy. The course focused more on health literacy than on the empowerment process though. There was a lack of support within the social and physical environment, to adequately support the use of new skills within everyday life. Challenges that have to be addressed when implementing health education for this target group in the future include improved adaptation to individual characteristics, pedagogical strategies that meet different learning styles and include participation in every part of the process and planning for well-functioning structures. To increase health-related behaviours it is important to improve health literacy as well as supporting the empowerment process. This might be achieved by creating an individualized supportive context in collaboration with caregivers and relatives.
Acknowledgements
The authors would like to thank the course leaders and the participants in the health courses for their participation.
Funding
The Public Health Fund, Stockholm County Council (HSN 0802-0339) and the Sävstaholm Foundation.
Conflict of interest statement
None declared.