





Abstract
Background: To accomplish the aims of public health practice and policy today, new forms of communication and education are being applied. Social media are increasingly relevant for public health and used by various actors. Apart from benefits, there can also be risks in using social media, but policies regulating engagement in social media is not well researched. This study examined European public health-related organizations’ social media policies and describes the main components of existing policies. Methods: This research used a mixed methods approach. A content analysis of social media policies from European institutions, non-government organizations (NGOs) and social media platforms was conducted. Next, individuals responsible for social media in their organization or projects completed a survey about their social media policy. Results: Seventy-five per cent of institutions, NGOs and platforms had a social media policy available. The primary aspects covered within existing policies included data and privacy protection, intellectual property and copyright protection and regulations for the engagement in social media. Policies were intended to regulate staff use, to secure the liability of the institution and social responsibility. Respondents also stressed the importance of self-responsibility when using social media. Conclusions: This study of social media policies for public health in Europe provides a first snapshot of the existence and characteristics of social media policies among European health organizations. Policies tended to focus on legal aspects, rather than the health of the social media user. The effect of such policies on social media adoption and usage behaviour remains to be examined.
Introduction
Public health aims to protect and promote health, prolong healthy life and prevent disease.1 Public health activities are increasingly using Web 2.0 technologies, particularly social media, to accomplish these aims. In social media, content is produced and published easily and quickly by individuals and organizations worldwide2 and facilitated by the adoption of technologies, such as portable computers and smartphones.3 The relevance of social media in public health is reflected in the growing number of scientific publications about social media and health, which increased from 55 publications in 2007 to 160 in 2011.4 Academics, policy makers, practitioners and patients use social media for networking, communicating information and research findings, patient empowerment and emergency preparedness efforts.5–8 In a recent Eurobarometer survey, respondents reported that having access to social networking and sharing sites is the most important reason for Europeans to disclose their private data, and 58% of the respondents reported to read privacy statements of the sites they are using.9 Yet, Europeans report concern about the tracking and recording of their online behaviours, and only 26% felt in complete control when using social networking sites.9
International activities in data collection and processing have raised governmental concern about online data protection, pressing for harmonized data protection legislation in all European countries. The European Data Protection Directive 95/46/EC covers the fundamental right to data protection and ensures the secure flow of personal data between the European Union’s (EU) member states. An updated Data Protection Directive, called the General Data Protection Regulation, is currently being discussed by the European Parliament.10 Compared with the existing Directive, the new Directive considers implications of technological progress for data protection and provides users with greater control over their personal data, more responsibilities for data processors and more conformity both inside and outside the EU.
The openness and interactivity available in social media suggest that a policy regarding conduct when using social media for public health purposes may be beneficial. Social media policies are ‘a set of statements, directives, regulations, laws and judicial interpretations that direct and manage the purposive and lawful use of social media by institutions and individuals, as members of the public and members of an organization’.11 Although companies, firms and institutions of public health and health-care providers are implementing social media policies that emphasize responsibility, disclosure of identity, truthful information and indication of own opinions,12 it is not known to what extent European health-related social media have policies for their use.
The aim of this study was to examine the social media policies of European public health organizations and describe the main components of such policies. Based on the findings, recommendations for developing social media policies that facilitate public health are discussed.
Methods
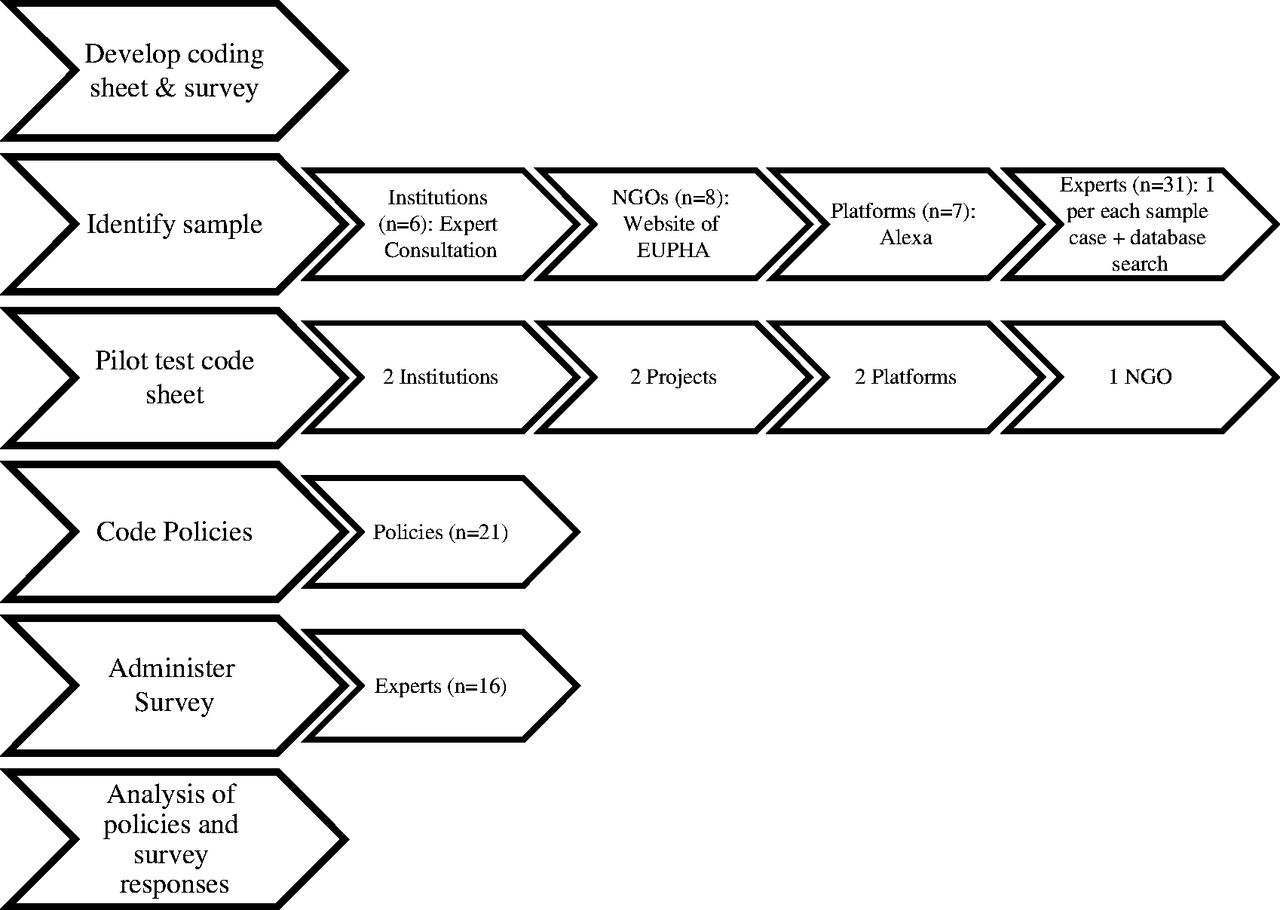
This research used a mixed methods approach, including a content analysis of policies and a survey of social media experts (see figure 1). Data were collected from May 2012 to June 2012. Results are reported in the aggregate; no individuals are identified nor are policy characteristics linked to their specific source when reporting the results.
Methodological process
Social Media policies were identified through an online search for European public health institutions, non-government organizations (NGOs) and social media platforms. Institutions were selected for inclusion if they used social media to communicate their activities. NGOs were selected by snowball sampling from the website of the European Public Health Alliance.13 Social media platforms were selected according to their global rank at Alexa, a web information company.14 When available, policies were obtained online. When not available online, the policy was requested by email. Both internal policies that guide the private and professional use of social media by staff and external policies guiding the use by the public were analysed (see Table 1).
Document titles used for the research
| Community Standards, Community Guidelines, |
| Pages Terms, Terms of Service, Terms of Use, Terms and Conditions, Code of Conduct, |
| Privacy Policy, Privacy Statement, |
| Copyright and Intellectual Property Right Policy, Copyright Infringement Notification, Copyright and Reprint Permission, |
| Data use Policy, |
| Social Media Strategy, |
| Legal Terms, (Important) Legal Notice, Disclaimer |
| Community Standards, Community Guidelines, |
| Pages Terms, Terms of Service, Terms of Use, Terms and Conditions, Code of Conduct, |
| Privacy Policy, Privacy Statement, |
| Copyright and Intellectual Property Right Policy, Copyright Infringement Notification, Copyright and Reprint Permission, |
| Data use Policy, |
| Social Media Strategy, |
| Legal Terms, (Important) Legal Notice, Disclaimer |
Document titles used for the research
| Community Standards, Community Guidelines, |
| Pages Terms, Terms of Service, Terms of Use, Terms and Conditions, Code of Conduct, |
| Privacy Policy, Privacy Statement, |
| Copyright and Intellectual Property Right Policy, Copyright Infringement Notification, Copyright and Reprint Permission, |
| Data use Policy, |
| Social Media Strategy, |
| Legal Terms, (Important) Legal Notice, Disclaimer |
| Community Standards, Community Guidelines, |
| Pages Terms, Terms of Service, Terms of Use, Terms and Conditions, Code of Conduct, |
| Privacy Policy, Privacy Statement, |
| Copyright and Intellectual Property Right Policy, Copyright Infringement Notification, Copyright and Reprint Permission, |
| Data use Policy, |
| Social Media Strategy, |
| Legal Terms, (Important) Legal Notice, Disclaimer |
Individuals from each institution, NGO and platform were invited to participate in the survey about the social media policy-making process. Additional experts, defined by having published an academic paper on health-related projects that used social media and social media experts in Europe, were identified through a search of Cochrane Library Database, Embase Medline, Web of Knowledge: Social Science Citation Index, Social Science Citation Index Expanded, PubMed, Cinhal and ERIC. Additionally, a hand search of journals that frequently publish on social media, health and data protection issues (according to a search in Web of Knowledge) was conducted (see table 2). The 26-item survey was administered in English online and by telephone and assessed the use of social media policies, the process of policy development, the extent to which public health was considered within policies and attitudes about the future of social media policy. The survey was available for 3 weeks, and reminders to complete were distributed to experts each week until they completed it or until the survey period closed.
Keywords for the literature review and identification of social media experts
| Keywords for database search | Keywords for the hand search of journals | Keywords for the search in the databases of the European Executive Agency for Health and Consumers and EU Community Research Development Information Service |
|---|---|---|
| [(‘social media’ OR ‘web2.0’ OR ‘web 2.0’ OR ‘social software’ OR ‘social web’ OR ‘social comput*’ OR ‘new media’ OR ‘interactive media’ OR ‘computer-based’) AND (‘health promotion’ OR ‘health communication’ OR ‘health education’ OR ‘health campaign*’ OR ‘health program*’ OR ‘health initiative’ OR ‘health care’ OR ‘healthcare’ OR ‘case stud*’ OR ‘study protocol*’ OR ‘health intervention’ OR ‘policy’ OR ‘regulation’ OR ‘guideline’ OR ‘toolkit’ OR ‘handbook’)] | (‘randomized controlled trial’ OR ‘case study’) AND (‘social media’ OR ‘web2.0’ OR ‘web 2.0’ OR ‘social software’ OR ‘social web’ OR ‘social comput*’ OR ‘new media’ OR ‘interactive media’ OR ‘computer-based’) | ‘social media’, ‘web2.0’, ‘web 2.0’, ‘social software’, ‘social web’, ‘social comput*’, ‘new media’, ‘interactive media’, or ‘computer-based’ |
| ‘Internet’ and ‘online’ were added in the search on health-focused databases; ‘health’ was added in searches on databases with a broader scientific focus |
| Keywords for database search | Keywords for the hand search of journals | Keywords for the search in the databases of the European Executive Agency for Health and Consumers and EU Community Research Development Information Service |
|---|---|---|
| [(‘social media’ OR ‘web2.0’ OR ‘web 2.0’ OR ‘social software’ OR ‘social web’ OR ‘social comput*’ OR ‘new media’ OR ‘interactive media’ OR ‘computer-based’) AND (‘health promotion’ OR ‘health communication’ OR ‘health education’ OR ‘health campaign*’ OR ‘health program*’ OR ‘health initiative’ OR ‘health care’ OR ‘healthcare’ OR ‘case stud*’ OR ‘study protocol*’ OR ‘health intervention’ OR ‘policy’ OR ‘regulation’ OR ‘guideline’ OR ‘toolkit’ OR ‘handbook’)] | (‘randomized controlled trial’ OR ‘case study’) AND (‘social media’ OR ‘web2.0’ OR ‘web 2.0’ OR ‘social software’ OR ‘social web’ OR ‘social comput*’ OR ‘new media’ OR ‘interactive media’ OR ‘computer-based’) | ‘social media’, ‘web2.0’, ‘web 2.0’, ‘social software’, ‘social web’, ‘social comput*’, ‘new media’, ‘interactive media’, or ‘computer-based’ |
| ‘Internet’ and ‘online’ were added in the search on health-focused databases; ‘health’ was added in searches on databases with a broader scientific focus |
Keywords for the literature review and identification of social media experts
| Keywords for database search | Keywords for the hand search of journals | Keywords for the search in the databases of the European Executive Agency for Health and Consumers and EU Community Research Development Information Service |
|---|---|---|
| [(‘social media’ OR ‘web2.0’ OR ‘web 2.0’ OR ‘social software’ OR ‘social web’ OR ‘social comput*’ OR ‘new media’ OR ‘interactive media’ OR ‘computer-based’) AND (‘health promotion’ OR ‘health communication’ OR ‘health education’ OR ‘health campaign*’ OR ‘health program*’ OR ‘health initiative’ OR ‘health care’ OR ‘healthcare’ OR ‘case stud*’ OR ‘study protocol*’ OR ‘health intervention’ OR ‘policy’ OR ‘regulation’ OR ‘guideline’ OR ‘toolkit’ OR ‘handbook’)] | (‘randomized controlled trial’ OR ‘case study’) AND (‘social media’ OR ‘web2.0’ OR ‘web 2.0’ OR ‘social software’ OR ‘social web’ OR ‘social comput*’ OR ‘new media’ OR ‘interactive media’ OR ‘computer-based’) | ‘social media’, ‘web2.0’, ‘web 2.0’, ‘social software’, ‘social web’, ‘social comput*’, ‘new media’, ‘interactive media’, or ‘computer-based’ |
| ‘Internet’ and ‘online’ were added in the search on health-focused databases; ‘health’ was added in searches on databases with a broader scientific focus |
| Keywords for database search | Keywords for the hand search of journals | Keywords for the search in the databases of the European Executive Agency for Health and Consumers and EU Community Research Development Information Service |
|---|---|---|
| [(‘social media’ OR ‘web2.0’ OR ‘web 2.0’ OR ‘social software’ OR ‘social web’ OR ‘social comput*’ OR ‘new media’ OR ‘interactive media’ OR ‘computer-based’) AND (‘health promotion’ OR ‘health communication’ OR ‘health education’ OR ‘health campaign*’ OR ‘health program*’ OR ‘health initiative’ OR ‘health care’ OR ‘healthcare’ OR ‘case stud*’ OR ‘study protocol*’ OR ‘health intervention’ OR ‘policy’ OR ‘regulation’ OR ‘guideline’ OR ‘toolkit’ OR ‘handbook’)] | (‘randomized controlled trial’ OR ‘case study’) AND (‘social media’ OR ‘web2.0’ OR ‘web 2.0’ OR ‘social software’ OR ‘social web’ OR ‘social comput*’ OR ‘new media’ OR ‘interactive media’ OR ‘computer-based’) | ‘social media’, ‘web2.0’, ‘web 2.0’, ‘social software’, ‘social web’, ‘social comput*’, ‘new media’, ‘interactive media’, or ‘computer-based’ |
| ‘Internet’ and ‘online’ were added in the search on health-focused databases; ‘health’ was added in searches on databases with a broader scientific focus |
Social media policies were analysed using a coding sheet developed by the research team that followed Cooper’s15 standardized method for coding in systematic reviews. It was developed inductively based on a pilot test with a selection of social media policies. Redundant or irrelevant codes were deleted, and additional codes were created to cover gaps noted in the piloted version. The final coding sheet consisted of 46 codes divided in the following six themes: (i) general information, (ii) scope of the policy (e.g., internal and external use), (iii) process of the policy, (iv) regulations, (v) legal aspects and (vi) public health. Findings from the content analysis and survey responses are reported together. First, we describe the extent to which social media policies exist and next describe the characteristics of such policies, including the process of policy development, the extent to which public health was considered within policies and attitudes about the future of social media policy.
Results
A total of 21 organizations (6 institutions, 8 NGOs and 7 platforms) and 31 experts were identified in the search (see table 3). Sixteen of the 31 social media experts completed the survey online or by telephone interview. Although we did not exclude any organization based on language, all collected documents were available in English.
Sample for policy analysis (N = 21)
| Institutions (n = 6) | Non-governmental organizations (n = 8) | Platforms (n = 7) |
|---|---|---|
|
|
|
| Institutions (n = 6) | Non-governmental organizations (n = 8) | Platforms (n = 7) |
|---|---|---|
|
|
|
Sample for policy analysis (N = 21)
| Institutions (n = 6) | Non-governmental organizations (n = 8) | Platforms (n = 7) |
|---|---|---|
|
|
|
| Institutions (n = 6) | Non-governmental organizations (n = 8) | Platforms (n = 7) |
|---|---|---|
|
|
|
Social media policies
Institutions, NGOs and platforms
All Institutions (n = 6) and platforms (n = 7) had external social media policies for the public use of their social media. Of the eight NGOs in the sample, 25% (n = 2) had a social media policy to regulate use by the public. An internal policy guiding their staff’s use of social media was found in 33% of the institutions, 25% of NGOs and 29% of social media platforms. Experts from NGOs and institutions that had not yet published an internal policy stated that internal policies for staff’s use of social media were either in draft stages or were to be implemented in the near future. Another respondent, speaking on behalf of a platform, stated to have a confidential social media policy for internal use, which therefore could not be analysed.
Social media experts
Fifty-six per cent of survey respondents had a social media policy, all of which had a policy regulating how staffs use their social media. The main reasons for having a social media policy were to regulate staff use, to secure the liability of the institution and social responsibility. Respondents that did not have a social media policy stated that such a policy was not perceived to be necessary.
Main components of social media policies
The most prevalent components in social media policies of public health institutions were a disclaimer (100%), copyright rule (83%) and privacy policy (83%). All NGOs’ policies included copyright and reprint regulations. Social media platform policies most commonly included a privacy policy (100%) and a set of community standards (86%). Other common items included copyright (86%), intellectual property rights regulations (71%) and limitations of liability (71%). Contact details were provided to users in 83% of institutions, 25% of NGOs and 86% of platforms policies. Of those who reported to have a social media policy in the survey (56%), all had a policy for staff use of social media for work purposes, all addressed the private use of social media by staff and one policy addressed external audiences. Overall, most social media experts were satisfied with their policy in terms of it being useful, important and comprehensible. They also reported that the effectiveness, comprehensiveness and ethical aspects of their policy were generally good.
Development process
The policy publication date was listed in 20% of policies, and 29% included information about being updated. Updates were typically made when an external event occurred or because of a predetermined schedule for updating the content. The content of the policies were often influenced by external factors (50%), with most influence coming from national and EU law. Legal frameworks and European directives influenced almost two-thirds of policies. Survey respondents reported that top management, managerial staff and executive staff or a combination most often designed policies, and the main influencers of policy were stakeholders and parent organizations.
Regulations
Regulation about data protection (66%) and stating when information is one’s own point of view (70%) were the most common types of regulations found in social media. Regulations about advertising and information about the ability to access, read and create content was found in all of the platform’s policies. The consequences for violating regulations were mentioned in 39% of policies and typically included the deletion of content or a user’s account and blocking future access. Rules for the deletion of content were present in 50% of policies.
Legal aspects
Every social media policy addressed and regulated privacy protection as well as explained the handling of personal data. Personally identifiable data were protected, but other data were stated to be used for various purposes. Platforms included information about the use of data for advertising purposes. The protection of intellectual property rights was covered in all policies, as well. The use of references, logos and trademarks was addressed by all policies of institutions and NGOs and by 86% of the platform policies.
Compliance with national law or any other laws and regulations was found in all policies. More than half of the platforms fell under US legislation but platforms mentioned the applicability of their policy within other national legislations. Two platforms mentioned their compliance to the US–EU Safe Harbour framework—an agreement between the EU and the USA to bridge their differences in private data protection rules.16 Liability addressed inappropriate use of content and associated consequences and was mentioned in four of the six institution policies and in one NGO policy.
The regulation with the least amount of coverage was the need to disclose a conflict of interest by users or moderators (10%). The professional degree of the moderator was mentioned in one NGO policy.
Public health
Public health was explicitly covered in 24% of the policies. Restrictions regarding the sharing of patient information were mentioned in 14%, and 45% mentioned that the social media content was not a replacement for professional advice. The opportunity to integrate individual health protection in the social media policy was present in all policies, e.g., by protection of health-related data or classifying health-related content. Public health was reported by experts to be the most relevant for their internal social media polices (to increase staff awareness of risks and benefits and to leverage their network and influence), in community standards and data protection. Mean, hateful or harassing content was prohibited in 54% of policies.
Attitudes towards the future of social media policy
Social media experts’ attitudes towards the future of social media policy were mixed. Experts mentioned the need to monitor social media by professionals, a need for more research in social media and their policies and that organizations currently regulate their social media use too much. Most respondents emphasized that regulations for social media contradict the values and principles of social media and could hinder the success of social media. Instead of regulations, self-responsibility by the health consumer was emphasized. Others responded that regulations would be useful, especially for data and privacy protection, but regulations were thought to be difficult to achieve on state- or EU-level, and the coordination between institutions would be needed.
Discussion
The findings suggest that public health institutions and platforms have social media policies and find them important. However, NGOs are lagging behind in policy implementation, although they perceive value in having a social media policy. Policies of platforms were more detailed and comprehensive, especially in terms of regulations, than the others. These findings are not surprising given that public health institutions and platforms are embedded in and more influenced by formal policy structures than NGOs typically are.
Although regulations for social media use are perceived to be beneficial, it is important to consider the open and dynamic nature of social media when designing such policies. Some of the social media experts in this study suggested that regulations are against the nature of social media and conflict with freedom of expression. They emphasized the importance of users’ self-responsibility and their capacity to retrieve and judge content correctly. However, it has also been suggested that social media, used for public health purposes, should address regulatory issues related to security, liability and privacy protection in social media.17,18 Social media policies can safeguard users and stimulate adequate security dimensions. Nevertheless, regulations should not restrict or complicate social media use.
In the spirit of social media and the importance of individual engagement in health, this may be an opportune moment to use social media to invite a people-centred approach to the formation of social media policy. This approach requires that all stakeholders, including lay public, practitioners, researchers and policy makers, have opportunities to communicate about needs and wants through a dialogue in social media. This dialogue may ultimately influence the development of social media policies for public health that are embraced by both the public and the provider of the social media.
This study is subject to several limitations. The sampling frame was intended to identify major European public health agencies, but some may have been inadvertently excluded. Although we did not intentionally exclude policies available in languages other than English, our search strategy may have prohibited policies in other languages from being identified. Further, some coding of policies may have been prone to subjectivity. Efforts to minimize the subjectivity included a pilot test of the coding and analysis procedures, and a survey of social media experts from the sample organizations allowed the confirmation of the themes derived in the coding of policies. A final limitation is that the invitation to participate in the survey, and the survey itself, were in English. This may partially explain why some experts did not respond to the survey invitation.
Conclusions
The findings obtained in this study provide a snapshot of health-related social media policy in Europe and can serve as a reference point in future studies on social media policy in public health. Such research might examine the role of specific components of a policy, such as having a certification (e.g., HONcode), privacy statements, referencing health claims and explicit mention of public health, on people’s willingness to share content. Understanding these policy components may assist in future policy development and to a better understanding of the importance of each component in facilitating public health through social media.
Conflicts of interest: None declared.
Research methods for the analysis of social media policies in a public health context have been developed and can serve researchers in future assessments of social media policy for public health.
Content of social media policies vary across categories and specificity and detail.
Harmonized data protection legislation, such as the reviewed European Data Protection Directive 95/46/EC can serve as a basis for internationally valid social media policies.
Future public health efforts that make use of social media are advised to have a policy about its use. Further research is needed to understand the implications of such policies on the public’s health and determinants of health (e.g., knowledge, self-efficacy, supportive environment).

{kind=link}
Comments
As somebody who has been using social media for years, I enjoyed the article by Fast et al on social media.[1]
Social networks can be a very valuable way of bringing people from overlapping disciplines together. I am a public health physician and former GP working primarily in health protection, and I am, of course also a citizen. I interact with other public health practitioners working in the same organisation as myself. I also liaise with academics in public health; and with practitioners and academics from public health, primary care and other settings both in the UK and abroad.
As a public health doctor, my first professional duty is to the population I serve.
Public health is, as readers of this journal are well aware, about much more than healthcare. As Virchow put it, "Medicine is a social science, and politics is nothing else but medicine on a large scale". So, as public health physicians, we inevitably dabble in politics.
Many of us work, however, in the public sector. As such we may be funded by a political system run by politicians whose beliefs about public health may be rather different from our own.
So the statement that "Policies were intended to regulate staff use, to secure the liability of the institution and social responsibility" struck a chord with me.
Recently there has been much debate about the value - or otherwise - of NHS Health Checks. I was a GP when "over-75 checks" were introduced as a result of a ministerial diktat (from Ken Clark, if I remember rightly), and was acutely aware of the resources that were wasted on these before they were quietly dropped.[2] NHS Health Checks were, similarly, introduced as a result of a ministerial diktat, and like other previous well-intentioned ideas, had also been controversial and widely debated.[3- 8]
When I tweeted a question about the evidence base for NHS health checks - commenting that I would like to think that the newly formed Public Health England was doing things because they were the right things to do and not just because a minister wanted them done - I was contacted by senior members of the organisation. I had committed a disciplinary offence, I was told, by breaching the organisation's social media policy. (In fact, the social media policy had not been agreed and ratified or even promulgated. At the time of writing the policy still hasn't been agreed; although it has been more widely promulgated by management as though it had been.)
The trade unions, including the BMA, have challenged the policy (and the way it has been promulgated prior to its agreement), and expect to see it changed.
Nevertheless, an attempt was made to prevent a well-informed professional from discussing a matter of public interest - presumably because they were questioning a politician's orders, and thereby, perhaps, annoying the holder of the organisation's purse-strings. It remains vital, however, that professionals - the people who, one would hope, know most about what is being discussed - are not excluded from airing their genuine concerns about how public money is spent because it is inconvenient to the politicians who fund the organisations they work for. If social media policies limit informed public debate about matters of legitimate public interest, they will harm the public interest.
REFERENCES
1. Fast I, S?rensen K, Brand H, Suggs LS. Social Media for Public Health: An Exploratory Policy Analysis. The European Journal of Public Health 2014. (http://eurpub.oxfordjournals.org/content/early/2014/06/18/eurpub.cku080.abstract). 2. Harris A. Health checks for people over 75. BMJ 1992;305(6854):599-600. (http://www.bmj.com/content/305/6854/599). 3. Holland W. Periodic Health Examination - A brief history and critical assessment. Eurohealth 2009;15(4):16-20. (http://www.lse.ac.uk/LSEHealthAndSocialCare/publications/eurohealth/eurohealth_volume_15_no_4_indiv.aspx). 4. Holland WW. Screening: reasons to be cautious [editorial]. Br Med J 1993;306:1222-3. 5. Krogsb?ll LT, J?rgensen KJ, Larsen CG, G?tzsche PC. General health checks in adults for reducing morbidity and mortality from disease: Cochrane systematic review and meta-analysis. BMJ 2012;345. (http://www.bmj.com/content/345/bmj.e7191). 6. McCartney M. Where's the evidence for NHS health checks? BMJ 2013;347:f5834 PMID: 24089427. (http://www.ncbi.nlm.nih.gov/pubmed/24089427). 7. Porter M. Health checks causing trouble. The Times Health News 2013; Updated 6 August; Accessed: 2013 (20 August): (http://www.thetimes.co.uk/tto/health/dr-mark-porter/article3835157.ece). 8. Wookey SL. Making the dilemma of universal health checks clear to patients. BMJ 2013;347. (http://www.bmj.com/content/347/bmj.f5230).
Conflict of Interest:
I am a BMA member and chair of my organisation's Local Negotiating Committee. I am a member of the NHS Action Party. I am an active user of Twitter.