



-
 PDF
PDF
- Split View
-
Views
-
Cite
Cite
Miquel À Mas, Marco Inzitari, Sergi Sabaté, Sebastià J Santaeugènia, Ramón Miralles, Hospital-at-home Integrated Care Programme for the management of disabling health crises in older patients: comparison with bed-based Intermediate Care, Age and Ageing, Volume 46, Issue 6, November 2017, Pages 925–931, https://doi.org/10.1093/ageing/afx099
Close - Share Icon Share

Abstract
to analyse the clinical impact of a home-based Intermediate Care model in the Catalan health system, comparing it with usual bed-based care.
quasi-experimental longitudinal study.
hospital Municipal de Badalona and El Carme Intermediate Care Hospital, Badalona, Catalonia, Spain.
we included older patients with medical and orthopaedic disabling health crises in need of Comprehensive Geriatric Assessment (CGA) and rehabilitation.
a CGA-based hospital-at-home Integrated Care Programme (acute care and rehabilitation) was compared with a propensity score matched cohort of contemporary patients attended by usual inpatient hospital care (acute care plus intermediate care hospitalisation), for the management of medical and orthopaedics processes. Main outcomes measures were: (a) Health crisis resolution (referral to primary care at the end of the intervention); (b) functional resolution: relative functional gain (functional gain/functional loss) ≥ 0.35; and (c) favourable crisis resolution (health + functional) = a + b. We compared between-groups outcomes using uni/multivariable logistic regression models.
clinical characteristics were similar between home-based and bed-based groups. Acute stay was shorter in home group: 6.1 (5.3–6.9) versus 11.2 (10.5–11.9) days, P < 0.001. The home-based scheme showed better results on functional resolution 79.1% (versus 75.2%), OR 1.62 (1.09–2.41) and on favourable crisis resolution 73.8% (versus 69.6%), OR 1.54 (1.06–2.22), with shorter length of intervention, with a reduction of −5.72 (−9.75 and −1.69) days.
in our study, the extended CGA-based hospital-at-home programme was associated with shorter stay and favourable clinical outcomes. Future studies might test this intervention to the whole Catalan integrated care system.
Introduction
Older adults with medical or surgical health crises need complex interventions due to the high prevalence of frailty, baseline disability and multimorbidity, which increase the risk of bad outcomes [1, 2]. In these patients, a hospital admission could be associated with adverse events, such as acute onset of disability or delirium [3–5]. These factors might limit their ability to resume life at home after the acute discharge, determining the need of multidisciplinary interventions to improve the transition until community reinsertion. These patients are not only exposed to higher risk of clinical adverse outcomes but also to longer hospital stay [6]. For these reasons, innovative integrated care admission avoidance and early discharge strategies have been validated in the last decades to improve clinical outcomes for several prevalent conditions, such as heart failure, COPD, infectious diseases, hip fracture and stroke, among others [7–15]. For selected patients, with these processes, hospital at home/hospital in the home provides acute or subacute treatment in a patient's residence for a condition that would normally require admission to hospital. It was found useful in the prevention of several geriatric conditions, as delirium and in the achievement of favourable functional outcomes [16–18].
In the territory of Catalonia (Spain), as well as in the UK, a strong bed-based Intermediate Care network was universally created and developed in the 80s and 90s. In patients with high and complex care needs, usual care includes acute hospitalisation and admission to bed-based Intermediate Care units. Based on the need to extend these Comprehensive Geriatric Assessment (CGA)-based interventions to the community, the implementation of home-based schemes is urged for our local health system [19]. In previous studies, our group presented preliminary results of an innovative CGA-based hospital-at-home model tailored to older patients with health crises leading to acute disability, developed as alternative care to usual inpatient care in an urban area in the north of Barcelona [20, 21]. From an initial sample of orthopaedic patients, attended by the hospital-at-home scheme and compared to an unmatched control sample of patients attended by conventional inpatient care, the home-based programme obtained favourable functional outcomes, specially in hip fracture patients [20]. A recent cost-effectiveness study, from the same cohort of orthogeriatric patients, showed that the model seems to enable lower direct costs [21].
The aim of this study was to analyse the results, in terms of effectiveness and efficiency, of this hospital-at-home model, extended from acute phase to post-acute phase and aimed to both Admission Avoidance (AA) and Early Supported Discharge (ESD), for older patients not only in orthopaedics but also in medical health crises leading to acute disability, as alternative care to usual inpatient care in our territory, by using a matching analysis method.
Methods
Design and setting
We conducted a quasi-experimental longitudinal study to compare clinical outcomes of two trajectories implemented at the Department of Geriatrics and Palliative Care of Badalona Serveis Assistencials, a public institution in an urban area in the North of Barcelona, Catalonia (Spain). Since 2010, older patients with acute disabling health crises from our Department can be oriented to two alternative Integrated Care Programmes (the new CGA-based hospital-at-home extended intervention or usual inpatient care). The study protocol was approved by the Ethics Committee of the Universitat Autònoma de Barcelona (reference number CEEAH-3003).
Participants and interventions
The study includes older patients needing any trajectory due to a health crisis during 3 years (2010–12). One group (intervention group) could receive either acute hospitalisation (for clinical instability due to medical processes or for surgical needs, such as orthopaedic surgery) plus home care provided based on the Hospital-at-home Integrated Care Programme through the innovative hospital-at-home unit (HHU), or direct access to HHU, if no needs of conventional acute admission were identified. The other group (control group) received usual inpatient care, including acute hospitalisation, if needed, plus admission to bed-based Intermediate Care unit (BBU).
All the patients presented an acute medical or surgical condition leading to acute disability, and needing CGA-based hospital-based care. Assignment to the intervention or control group was not randomised, but based on the availability of resources, on carer availability and on patient acceptance. The only differential requirement to be admitted to the HHU (versus the BBU) was having a 24 h caregiver with enough physical and cognitive capacity to assure health care at home, and that patient and caregiver gave consent. If a 24 h caregiver was not available, or the patient did not consent to be assigned discharged home within the HHU, a BBU referral was activated. In both cases, of discharge from acute care to HHU and BBU, as well as in case of direct activation of CGA-based resources (from the community or the Emergency Department) patients had to show hemodynamic stability, without requirements of 24 h follow-up in an acute ward. Having a diagnosis of cognitive impairment and/or living in a care home were not exclusion criteria for both units.
Both groups (intervention and control) received the same protocol based on CGA to develop an individualised care plan, reviewed in weekly multidisciplinary meetings. The care plan was centred on managing acute changes in geriatric syndromes and on functional improvement, to care for functional loss determined by the health crisis, plus individual needs. HHU and BBU care included managing the needs of high-risk patients during the rehabilitation process, with acute treatment if needed (e.g. treating infections, heart failure or other acute conditions) by its specialised health staff using technology (blood and microbiologic test and ECG, and radiology from the acute hospital), when necessary [20]. HHU staff included a geriatrician and two nurses (full time), from the department of Geriatrics, plus a consultant physical medicine and rehabilitation specialist, four physiotherapists and an occupational therapist (part time), from community services. Staff from the same disciplines provided full time care at BBU.
Data from 91 individuals in the intervention group and 276 individuals in the control group of this study, all with orthopaedic conditions, were included in a previous cost-effectiveness analysis [21], whereas, from the same sample of orthopaedic patients, 69 in the intervention group and 201 in the control group were included in a pilot unmatched analysis to explore functional evolution [20].
Data collection
Data were extracted from the electronic health records of the hospital, by administrative staff. We included age, gender, diagnostic group (medical or orthopaedic), ESD or AA strategy, and length of acute stay (for ESD strategy), and main clinical characteristics of the patients. We collected: baseline Barthel index (BI) Granger's version [22], BI at admission to each unit, functional loss at admission to each unit (calculated as baseline BI – BI at admission), Charlson comorbidity index [23], and number of geriatric syndromes, including presence of cognitive impairment, prevalent delirium or mood disorder. At discharge, BI, discharge destination and length of stay were recorded. This allowed computing functional gain (BI at discharge – BI at admission) [24–26].
Outcomes
Main outcomes at the end of the intervention were:
Health crisis resolution: discharge to primary care at the end of the intervention.
Functional resolution: functional gain ≥ of 35% of functional loss, that means that the patient has recovered at least one third of the functional loss observed [24–26].
Favourable crisis resolution (health + functional): a + b.
Other secondary outcomes were: length of intervention (length of stay in the unit) in days, BI at discharge, rehabilitation efficiency (RE = functional gain/length of stay; RE ≥0.5 was considered moderate/high RE for each unit) [24–26], and discharge destination.
Analysis
Categorical variables are presented as absolute numbers and percentages, and continuous variables are reported as means (95% confidence interval [CI]) or median (interquartile range).
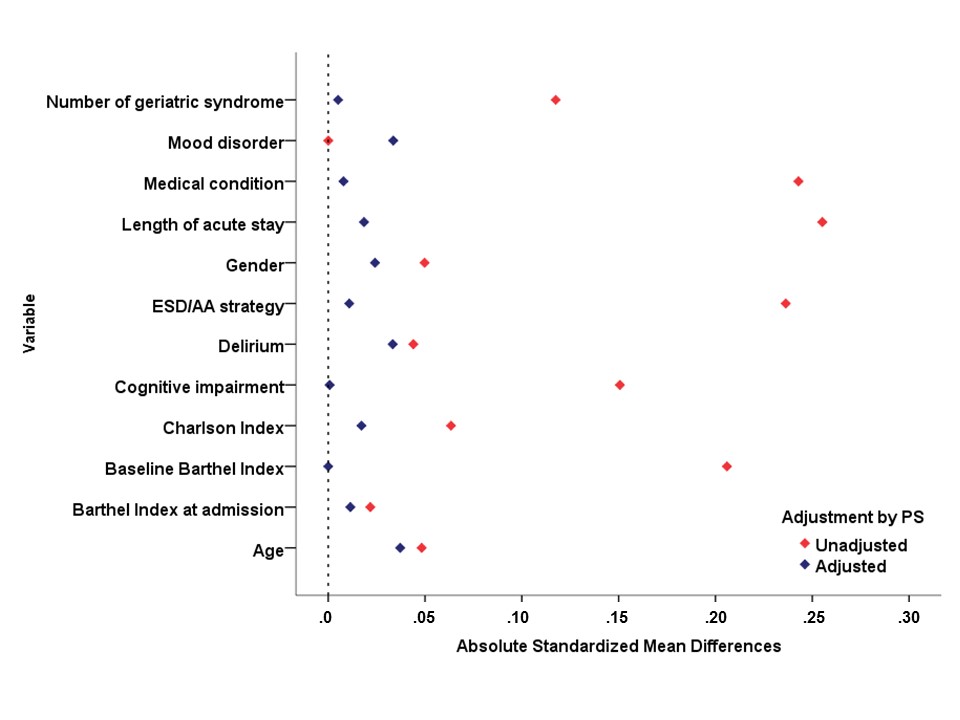
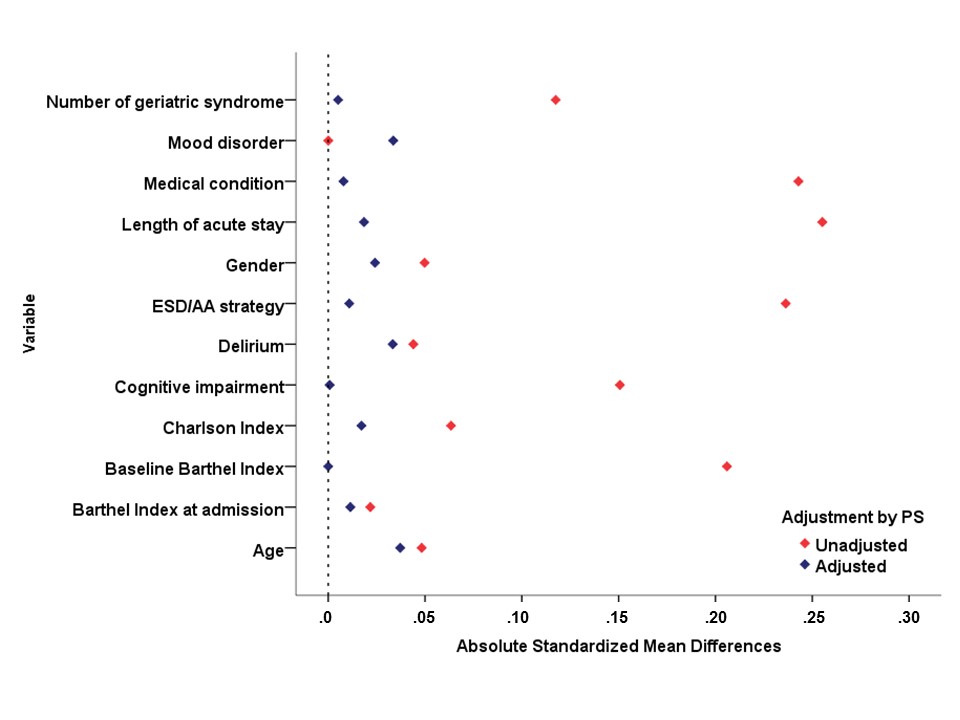
A propensity score (PS) method was employed to balance the distribution of measured covariates between the two groups of patients receiving treatment at hospital (BBU) or at home (HHU). The PS, reflecting the likelihood of receiving treatment at home, was derived from a nonparsimonious multiple logistic regression that included all predictor variables that might be related to treatment at home or potential confounders for endpoints. These variables were demographic (age, gender) and characteristics such as diagnostic group, ESD/AA strategy, length of acute stay, baseline BI, BI at admission to each unit, Charlson index, cognitive impairment, delirium, mood disorder and number of geriatric syndromes. Thus, the PS generated for each patient, based on the individual's covariate values, reflected the likelihood that the patient would receive treatment at home. The goodness-of-fit diagnostic for the model was calculated by standardised mean differences before and after adjustment [27]. Afterwards, a new logistic regression model with treatment (hospital/home) as the independent variable and PS as a covariate (covariate-adjustment) was constructed to evaluate each end point (adjusted odds ratio).
Additionally, the association between treatment at home (adjusted by PS) and Barthel at discharge, and duration of intervention was evaluated by means of linear regression.
Both the unadjusted and PS–adjusted odds ratios and 95% CIs were estimated for each regression analysis. Two-tailed P < 0.05 was considered to denote significant differences. The Figure 1 shows absolute standardised mean differences and adjustment by PS (see Supplementary data, Figure Appendix 1, available at Age and Ageing online).
Statistical analysis was performed with the SPSS software package (IBM SPSS Statistics 20, Chicago, IL).
Results
We included a total of 849 subjects (244 in the HHU and 605 in the BBU). Mean age was 83.2, 72% females, 73.4% referred from acute wards (ESD strategy), main diagnostic was medical in 43% versus orthopaedics 57%. Baseline characteristics of the sample, by groups are shown in Table 1. Baseline functional status pre-event was worst for the HHU group (due to higher prevalence of cognitive impairment and other geriatric syndromes). Functional loss due to the health crisis was higher in the BBU. Main outcomes of the whole sample were: health crisis resolution in 79% and functional resolution in 76.3% of the sample. Discharge destination was: community (with GP follow-up) 79%, acute hospital 7.4%, long term care setting 9.8% and death 3.8%. For patients referred from acute wards (ESD strategy), a shorter length of acute stay was found for the HHU group: 6.1 (5.3–6.9) versus 11.2 (10.5–11.9) days.
Demographical and clinical characteristics by group
| . | HHU, n = 244 . | BBU, n = 605 . | P value . |
|---|---|---|---|
| Age (y), mean (95% CI) | 83.8 (82.9–84.6) | 83 (82.4–83.6) | 0.160 |
| Gender (female), n (%) | 167 (68.4) | 444 (73.4) | 0.152 |
| Main diagnostic Medical (versus Orthopaedics), n (%) | 152 (62.3) | 213 (35.2) | <0.001 |
| ESD/AA strategy (%) | 56.6/43.4 | 80.2/19.8 | <0.001 |
| Length of acute stay (d), median (IQR) | 6.1 (5.3–6.9) | 11.2 (10.5–11.9) | <0.001 |
| Baseline Barthel index, median (IQR) | 75.2 (72.4–77.9) | 83.9 (82.2–85.6) | <0.001 |
| Barthel index at admission, median (IQR) | 41.5 (38.4–44.6) | 42.6 (40.7–44.5) | 0.527 |
| Charlson index, median (IQR) | 2 (1–3) | 2 (1–3) | 0.467 |
| Number of geriatric syndromes, median (IQR) | 5 (4–6) | 4 (3–6) | <0.001 |
| Cognitive impairment, n (%) | 101 (41.4) | 157 (26) | <0.001 |
| Delirium, n (%) | 41 (16.8) | 81 (13.4) | 0.197 |
| Mood disorder, n (%) | 48 (19.7) | 119 (19.7) | 1.000 |
| Functional loss, median (IQR) | 33.7 (31.5–35.9) | 41.1 (39.5–42.7) | <0.001 |
| . | HHU, n = 244 . | BBU, n = 605 . | P value . |
|---|---|---|---|
| Age (y), mean (95% CI) | 83.8 (82.9–84.6) | 83 (82.4–83.6) | 0.160 |
| Gender (female), n (%) | 167 (68.4) | 444 (73.4) | 0.152 |
| Main diagnostic Medical (versus Orthopaedics), n (%) | 152 (62.3) | 213 (35.2) | <0.001 |
| ESD/AA strategy (%) | 56.6/43.4 | 80.2/19.8 | <0.001 |
| Length of acute stay (d), median (IQR) | 6.1 (5.3–6.9) | 11.2 (10.5–11.9) | <0.001 |
| Baseline Barthel index, median (IQR) | 75.2 (72.4–77.9) | 83.9 (82.2–85.6) | <0.001 |
| Barthel index at admission, median (IQR) | 41.5 (38.4–44.6) | 42.6 (40.7–44.5) | 0.527 |
| Charlson index, median (IQR) | 2 (1–3) | 2 (1–3) | 0.467 |
| Number of geriatric syndromes, median (IQR) | 5 (4–6) | 4 (3–6) | <0.001 |
| Cognitive impairment, n (%) | 101 (41.4) | 157 (26) | <0.001 |
| Delirium, n (%) | 41 (16.8) | 81 (13.4) | 0.197 |
| Mood disorder, n (%) | 48 (19.7) | 119 (19.7) | 1.000 |
| Functional loss, median (IQR) | 33.7 (31.5–35.9) | 41.1 (39.5–42.7) | <0.001 |
HHU = hospital-at-home unit; BBU = bed-based unit; CI = confidence interval; IQR = interquartile range; ESD = early supported discharge; AA = admission avoidance.
Demographical and clinical characteristics by group
| . | HHU, n = 244 . | BBU, n = 605 . | P value . |
|---|---|---|---|
| Age (y), mean (95% CI) | 83.8 (82.9–84.6) | 83 (82.4–83.6) | 0.160 |
| Gender (female), n (%) | 167 (68.4) | 444 (73.4) | 0.152 |
| Main diagnostic Medical (versus Orthopaedics), n (%) | 152 (62.3) | 213 (35.2) | <0.001 |
| ESD/AA strategy (%) | 56.6/43.4 | 80.2/19.8 | <0.001 |
| Length of acute stay (d), median (IQR) | 6.1 (5.3–6.9) | 11.2 (10.5–11.9) | <0.001 |
| Baseline Barthel index, median (IQR) | 75.2 (72.4–77.9) | 83.9 (82.2–85.6) | <0.001 |
| Barthel index at admission, median (IQR) | 41.5 (38.4–44.6) | 42.6 (40.7–44.5) | 0.527 |
| Charlson index, median (IQR) | 2 (1–3) | 2 (1–3) | 0.467 |
| Number of geriatric syndromes, median (IQR) | 5 (4–6) | 4 (3–6) | <0.001 |
| Cognitive impairment, n (%) | 101 (41.4) | 157 (26) | <0.001 |
| Delirium, n (%) | 41 (16.8) | 81 (13.4) | 0.197 |
| Mood disorder, n (%) | 48 (19.7) | 119 (19.7) | 1.000 |
| Functional loss, median (IQR) | 33.7 (31.5–35.9) | 41.1 (39.5–42.7) | <0.001 |
| . | HHU, n = 244 . | BBU, n = 605 . | P value . |
|---|---|---|---|
| Age (y), mean (95% CI) | 83.8 (82.9–84.6) | 83 (82.4–83.6) | 0.160 |
| Gender (female), n (%) | 167 (68.4) | 444 (73.4) | 0.152 |
| Main diagnostic Medical (versus Orthopaedics), n (%) | 152 (62.3) | 213 (35.2) | <0.001 |
| ESD/AA strategy (%) | 56.6/43.4 | 80.2/19.8 | <0.001 |
| Length of acute stay (d), median (IQR) | 6.1 (5.3–6.9) | 11.2 (10.5–11.9) | <0.001 |
| Baseline Barthel index, median (IQR) | 75.2 (72.4–77.9) | 83.9 (82.2–85.6) | <0.001 |
| Barthel index at admission, median (IQR) | 41.5 (38.4–44.6) | 42.6 (40.7–44.5) | 0.527 |
| Charlson index, median (IQR) | 2 (1–3) | 2 (1–3) | 0.467 |
| Number of geriatric syndromes, median (IQR) | 5 (4–6) | 4 (3–6) | <0.001 |
| Cognitive impairment, n (%) | 101 (41.4) | 157 (26) | <0.001 |
| Delirium, n (%) | 41 (16.8) | 81 (13.4) | 0.197 |
| Mood disorder, n (%) | 48 (19.7) | 119 (19.7) | 1.000 |
| Functional loss, median (IQR) | 33.7 (31.5–35.9) | 41.1 (39.5–42.7) | <0.001 |
HHU = hospital-at-home unit; BBU = bed-based unit; CI = confidence interval; IQR = interquartile range; ESD = early supported discharge; AA = admission avoidance.
Both groups obtained satisfactory results of health crisis resolution in 8/10 cases, with low percentage of readmission or death, as shown in Table 2 (unadjusted results). The hospital-at-home programme (HHU) obtained similar outcomes on functional resolution and on favourable crisis resolution, compared to usual bed-based strategy (BBU). However, when results were adjusted by PS model, HHU was associated with favourable crisis resolution (health and functional) [OR = 1.54 (1.06–2.22)], and with shorter intervention stay (mean difference: −5.72 days (−9.75 to −1.69)). The goodness of fit of the PS model was appropriate since the absolute standardised mean differences after adjustment tended to 0 (see Supplementary data, Appendix 1, available at Age and Ageing online).
Main outcomes by group
| . | HHU, n = 244 . | BBU, n = 605 . | P value . |
|---|---|---|---|
| Length of stay in the unit (d); mean (95% CI) | 46.6 (43.9–49.2) | 55.5 (52.9–57.2) | <0.001 |
| Barthel Index at discharge, median (IQR) | 67.9 (64.3–71.6) | 69.7(67.1–72.2) | 0.036 |
| Health crisis resolution, n (%) | 192 (78.7) | 479 (79.2) | 0.926 |
| Functional resolution, n (%) | 193 (79.1) | 455 (75.2) | 0.247 |
| Favourable crisis resolution (health + functional), n (%) | 180 (73.8) | 421 (69.6) | 0.243 |
| Rehabilitation efficiency, mean (95% CI) | 0.60 (0.53–0.66) | 0.52 (0.46–0.58) | 0.292 |
| Discharge destination, n (%) | 0.027 | ||
| Community | 192 (78.7) | 479 (79.2) | |
| Acute care unit | 26 (10.7) | 37 (6.1) | |
| Long term care setting | 22 (9) | 61 (10.1) | |
| Death | 4 (1.6) | 28 (4.6) |
| . | HHU, n = 244 . | BBU, n = 605 . | P value . |
|---|---|---|---|
| Length of stay in the unit (d); mean (95% CI) | 46.6 (43.9–49.2) | 55.5 (52.9–57.2) | <0.001 |
| Barthel Index at discharge, median (IQR) | 67.9 (64.3–71.6) | 69.7(67.1–72.2) | 0.036 |
| Health crisis resolution, n (%) | 192 (78.7) | 479 (79.2) | 0.926 |
| Functional resolution, n (%) | 193 (79.1) | 455 (75.2) | 0.247 |
| Favourable crisis resolution (health + functional), n (%) | 180 (73.8) | 421 (69.6) | 0.243 |
| Rehabilitation efficiency, mean (95% CI) | 0.60 (0.53–0.66) | 0.52 (0.46–0.58) | 0.292 |
| Discharge destination, n (%) | 0.027 | ||
| Community | 192 (78.7) | 479 (79.2) | |
| Acute care unit | 26 (10.7) | 37 (6.1) | |
| Long term care setting | 22 (9) | 61 (10.1) | |
| Death | 4 (1.6) | 28 (4.6) |
HHU = hospital-at-home unit; BBU = bed-based unit; CI = confidence interval; IQR = interquartile range; functional resolution = functional gain >35% of functional loss.
Main outcomes by group
| . | HHU, n = 244 . | BBU, n = 605 . | P value . |
|---|---|---|---|
| Length of stay in the unit (d); mean (95% CI) | 46.6 (43.9–49.2) | 55.5 (52.9–57.2) | <0.001 |
| Barthel Index at discharge, median (IQR) | 67.9 (64.3–71.6) | 69.7(67.1–72.2) | 0.036 |
| Health crisis resolution, n (%) | 192 (78.7) | 479 (79.2) | 0.926 |
| Functional resolution, n (%) | 193 (79.1) | 455 (75.2) | 0.247 |
| Favourable crisis resolution (health + functional), n (%) | 180 (73.8) | 421 (69.6) | 0.243 |
| Rehabilitation efficiency, mean (95% CI) | 0.60 (0.53–0.66) | 0.52 (0.46–0.58) | 0.292 |
| Discharge destination, n (%) | 0.027 | ||
| Community | 192 (78.7) | 479 (79.2) | |
| Acute care unit | 26 (10.7) | 37 (6.1) | |
| Long term care setting | 22 (9) | 61 (10.1) | |
| Death | 4 (1.6) | 28 (4.6) |
| . | HHU, n = 244 . | BBU, n = 605 . | P value . |
|---|---|---|---|
| Length of stay in the unit (d); mean (95% CI) | 46.6 (43.9–49.2) | 55.5 (52.9–57.2) | <0.001 |
| Barthel Index at discharge, median (IQR) | 67.9 (64.3–71.6) | 69.7(67.1–72.2) | 0.036 |
| Health crisis resolution, n (%) | 192 (78.7) | 479 (79.2) | 0.926 |
| Functional resolution, n (%) | 193 (79.1) | 455 (75.2) | 0.247 |
| Favourable crisis resolution (health + functional), n (%) | 180 (73.8) | 421 (69.6) | 0.243 |
| Rehabilitation efficiency, mean (95% CI) | 0.60 (0.53–0.66) | 0.52 (0.46–0.58) | 0.292 |
| Discharge destination, n (%) | 0.027 | ||
| Community | 192 (78.7) | 479 (79.2) | |
| Acute care unit | 26 (10.7) | 37 (6.1) | |
| Long term care setting | 22 (9) | 61 (10.1) | |
| Death | 4 (1.6) | 28 (4.6) |
HHU = hospital-at-home unit; BBU = bed-based unit; CI = confidence interval; IQR = interquartile range; functional resolution = functional gain >35% of functional loss.
Discussion
In our sample of older patients with disabling health crises attended by the hospital-at-home Integrated Care Programme, the home-based scheme had at least the same crisis resolution capacity, but reducing days of hospitalisation, compared to a usual bed-based contemporary cohort. Moreover, these results were found associated with a shorter length of intervention, and with better functional outcomes at discharge for the home group.
Based on a previous subanalysis of a meta-analysis on early discharge hospital-at-home for older patients with a mix of conditions [7], it was not clear that home-based schemes could reduce total days of care (hospital plus hospital-at-home). Our work suggests that a hospital-at-home scheme linked to a hospital-based department of geriatrics, working in an integrated care scenario, can reduce days of hospitalisation without increasing length of hospital-at-home stay (compared to the control cohort). It supports our hypothesis that developing a CGA-based protocol at home, with a full-time geriatrician integrated in the multidisciplinary team, could have impact on the earlier resolution of the health crises attended by the hospital-at-home team.
The current evidence on hospital-at-home interventions includes a limited number of RCT classified as ESD and AA schemes, from the UK and other countries [7–9]. In most papers, the role of standardised CGA in the intervention is not clear. Most schemes focused on interventions designed for the short-term phase of the health crisis; it seems that the rehabilitation phase is not included in some of the described interventions [19]. Few studies showed positive results on function and other related outcomes (as length to readmission) at follow up [10–11]. Other schemes focused on early discharge and rehabilitation, for paradigmatic disabling conditions as stroke, but these schemes do not have the capacity to provide acute care at home if needed [15]. In some cases, these resources are linked to a hospital but in other cases they are linked to community teams and primary care. There is not a homogeneous home-based Intermediate Care model, depending on the context and evolution of each single local region where it was implemented [19]. In this sense, the development of our model was based on the need to provide acute care and rehabilitation by a home-based alternative scheme to inpatient care. The model was built on the idea of adapting care models and protocols of geriatric wards to the community, and of promoting continuity of care for the ‘whole’ crisis, earlier from acute phase to community reinsertion.
Previous studies, by Caplan et al. [28] and Cunliffe et al. [29], have evaluated similar models, although more specialised full-time geriatrician involvement characterises our intervention. The Sydney group [28] found home rehabilitation after acute hospitalisation associated with a lower risk of delirium, greater patient satisfaction, lower cost and more efficient hospital bed use. The Nottingham group [29], found that patients attended by the home-based service spent fewer days in hospital at 3 months, with better functional scores and better results in general health questionnaire scores. Our team had the possibility to provide intensive health care from specialised hospital staff (up to 2–3 health visits per day if necessary, depending on patient's needs). At home, complex conditions (as severe functional loss leading to immobility, delirium or behavioural symptoms) could be managed by specialist nurses and therapists from the multidisciplinary team. The care process could be tailored to each patient, adapting individualised sessions/home visits to patients’ profiles (previous level of disability, multimorbidity, cognitive status, etc.). Interventions could be modified depending on the health status of the patients during the functional trajectory of recovery (e.g. evolution of delirium or fluctuations of cognitive status). It was considered relevant because high risk of negative results based on baseline characteristics of these patients (frailty, baseline disability and presence of multiple chronic conditions). Old age, the presence of cognitive impairment, delirium and prevalence of geriatric conditions, could led to readmission and institutionalisation, if a comprehensive approach is not provided in patients in need of rehabilitation. In our study, the health staff came from the same hospital department as the BBU, and they had the same capability for managing multiple morbidities, persistent acute conditions after hospital discharge (e.g. delirium), and provide acute treatment (e.g. low-risk infections, heart failure and other acute illnesses with a good prognosis), without readmission to an acute unit in most cases. A previous analysis of our integrated care model in the community found good results of our programme in hip fracture patients [20].
The favourable results of our hospital-at-home integrated care unit, compared to the bed-based scheme, could be expected based on previous hospital-at-home research. Leff et al. [18] and Caplan et al. [17, 28] demonstrated favourable functional outcomes, based on instrumental activities of daily living, of home-based care versus inpatient care. As suggested by several groups, at home multidisciplinary interventions can be tailored to each individual case [8].
The non-randomisation might be considered a limitation. Some authors suggest that approaches other than RCT are useful to evaluate complex clinical interventions in some innovative complex schemes (e.g. implementing ESD programmes in the clinical practice for the treatment of stroke or other acutely disabling conditions) [15]. In this sense, the PS method validates the hypothesis of comparable samples according to the collected variables in our study. The limitation of PS is that the balance of observed covariates does not guarantee balance of unobserved covariates (as the impact of illness acuity or social support). We assume that omitting an unknown confounder from the PS model could produce some biases. Another relevant aspect of non-randomisation could be the presence of a 24 h caregiver as an inclusion criterion of the experimental intervention. From a clinical perspective, the criterion of availability of a 24 h caregiver at the beginning of the clinical process does not seem a key factor. For the inpatient sample (patients with good baseline functional status suffering a medical or orthopaedical health crisis with good functional prognosis), we hypothesised that a health crisis resolution should be based on the clinical intervention, not in social support at home. Lack of data on pre-admission social status could be another limitation of the study. Although the HHU group have lower functional status at admission there is a greater functional drop in the BBU group which could correlate to acuity of illness not measured in this study. Strengths include that we are presenting a'real world’ intervention, not limited to an experimental setting but currently implemented and part of available system's option, the pragmatic approach of not excluding patients for having cognitive impairment or living in a care home, and the availability of complete clinical data, based on CGA at admission to both units.
Our hospital-at-home model not only focuses on early discharge or admission avoidance strategies for acute treatment and clinical stabilisation but also extends the CGA-based intervention to the rehabilitation phase, tailoring the intervention to the ‘whole’ (clinical and functional) resolution of the health crisis. In this sense, it is an opportunity to deliver patient-centred care plans that finish with patient community reinsertion, with a very flexible approach which might be adapted to the need of patients’ care within a territory.
Future research directions might include larger randomised studies, multicentre designs, and other evaluation of economic or cost-effectiveness aspects of this type of intervention.
In conclusion, from our local ‘real life’ pragmatic approach, we support there is a role for new integrated care strategies in the community. We could adapt CGA-based interventions from inpatient to a HHU, with efficient clinical results, compared with usual CGA-based hospital care. If confirmed by further studies it might be a good point for starting hospital-at-home integrated care schemes in our national health system.
Bed-based Intermediate Care works as usual care for admission avoidance and early discharge strategies in some countries.
In some regions, home-based Intermediate Care is fragmented between hospital-at-home teams and reablement schemes.
We present a quasi-experimental study matching a hospital-at-home scheme with usual inpatient units for the care of disabling health crises.
The home-based scheme showed better results on favourable crisis resolution, with shorter stay than bed-based units.
Supplementary data
Supplementary data mentioned in the text are available at Age and Ageing online.
Acknowledgements
The development and analysis of the Hospital-at-home Integrated Care Programme is the centre of the PhD project of Dr Miquel Àngel Mas (with Dr Marco Inzitari, from Universitat Autònoma de Barcelona, as a Director, and Dr Ramón Miralles, as a Tutor).
The Hospital-at-home Integrated Care Programme received the certification of Innovative Experience in 2015 by the Observatory of Innovation in Healthcare Management from the Department of Health of Catalonia (Spain).
We would like to thank Sonia Garcia for her support in data collection.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
Comments